Diagnostic info you just can't see elsewhere
September 2010 | dentalproductsreport.com Clinical 360°: Implants The take-aways CBCT is crucial for creating excellence in the esthetic zone. When multiple implants are being planned, it can offer invaluable information. Dianostic info you just can't see elsewhere Part III illustrates two implant cases where CBCT provides valuable information for treatment planning. by Dr. Michael Tischler
September 2010 | dentalproductsreport.com
Clinical 360°: Implants
The take-aways
- CBCT is crucial for creating excellence in the esthetic zone.
- When multiple implants are being planned, it can offer invaluable information.
Dianostic info you just can't see elsewhere
Part III illustrates two implant cases where CBCT provides valuable information for treatment planning.
by Dr. Michael Tischler
At a glance




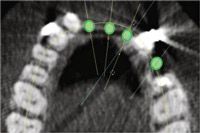





FIGS. 1-4 Clinical view of maxillary arch showing missing teeth (Fig. 1). Axial view showing planned implants in area 8, 9, 10, 12 (Fig. 2). Cross-sectional view showing buccal and lingual bone for implant placement (Fig. 3). Periapical view showing spacing of implants post placement (Fig. 4).



Click here for a slideshow of the entire case.
The set-up
“Dr. Tischler uses two cases, one involving implant placement in the esthetic zone and the other a complex case that necessitated osseous grafting and multiple implants, to illustrate the benefits of using CBCTs to optimize the planning and placement of implants. The cross-sectional and 3D views obtained provide pre-operative diagnostic information that would be otherwise unavailable.”
-Dr. BRIEN HARVEY, TEAM LEAD
This article concludes a three-part series on treatment planning for dental implants with cone beam computed tomography (CBCT). Part one (DPR, March) outlined the basics of CBCT imaging principles and the relevance to treatment planning for dental implants. The importance of a clinician using the available CT imaging processing companies was made evident, with an emphasis on the team approach. Part two (DPR, June) brought in clinical relevance with examples of how every area of the mouth can require CBCT imaging for clinical success and medical legal protection when placing dental implants. In part two, the importance of CBCT for bone grafting also was emphasized. Bone grafting is the foundation of implant dentistry.
This last part of the series covers CBCT imaging for implant placement in the esthetic zone as well as in larger implant cases. It will be shown how CBCT is crucial for creating excellence in the esthetic zone, due to the need for precision in that area of the mouth. It will also be clear how important CBCT is when doing multiple implants, from both a surgical and prosthetic standpoint.
CBCT in the esthetic zone
Successfully placing and restoring dental implants in the anterior maxillary esthetic zone offers one of the most challenging tasks in dentistry. Not only is a clinician dealing with the subjective issues of cosmetic dentistry, but also the challenges of hard- and soft-tissue changes are in play. These challenges are compounded when a patient’s lip line is high, only increasing the esthetic demands. Often before placing an implant in the anterior region, site development needs to happen to achieve ideal esthetics. This site development might require bone grafting and soft-tissue grafting or shaping. A CBCT often can offer information that shows when, where and if grafting procedures are needed.
26% of respondents said they would add CBCT to their practice if money were not an issue, which was the most popular choice. Source: DPR August 2010 Technology Census.
When a patient presents edentulous in the anterior region, a CT is needed to ascertain the present bone height and width, implant spacing and relative position to the adjacent teeth. Figure 1 shows how a patient presented, edentulous in areas number 8, 9, 10 and 12.
One of the most important parameters in planning for ideal esthetics in the anterior region is to space the implants accordingly. The literature suggests a minimum of 3 mm between implants and 2 mm between an implant and a natural tooth. Through analysis of a CBCT, the correct spacing can be planned. The axial view from a CBCT shows spacing of implants (Fig. 2).
A surgical guide stent created from the CBCT information can be made, and this would assist implant placement, especially with clinicians early in their implant experience. In this case because of the adjacent teeth offering a relative position, a stent was not used. Another important issue in the anterior region is to have adequate buccal and lingual width. If there is bone loss on the facial of a dental implant, there is the potential for gum loss. This is because it is the bone that supports soft tissue and the papillae. Figure 3 shows a cross-sectional view and the correct amount of bone needed both facially and lingually.
A periapical radiograph confirms the implant placement and spacing as per the plan from the CBCT (Fig. 4). The final prosthesis shows the esthetics that can be obtained through correct planning with a CBCT (Fig. 5). Unless the spacing between implants is correct, the soft tissue may not form esthetically. Papilla need adequate blood supply to maintain their form. Many factors such as gingival biotype, tissue height and tooth form are factors to implant success in the esthetic zone. The information gained from a CBCT offers the fundamental principles of spacing and positioning. Without these parameters, success in this region is not possible.
Using for larger, complex cases
When multiple implants are being planned, a CBCT can offer invaluable information with regards not only to spacing issues but also to the proximity to the maxillary sinuses, mandibular foramen, mental foramen, lingual fossa and many other important anatomical structures.
When a patient presents with a hopeless bridge, a panograph is a good start to assess the basic bone level for future implant placement. Figure 6 shows the condition on the panograph in which the patient in this case presented with a failing maxillary fixed prosthesis. Figure 7 shows the clinical condition of the prosthesis and the unesthetic appearance of it.
When teeth are being extracted, a CBCT can accurately assess the remaining bone after tooth removal. Figure 8 shows a 3D view in Materialise’s SimPlant (materialise.com/dental), which clearly shows deficient areas in the ridge for implant placement. The Cross sectional and axial view of the SimPlant program also show substantial bone loss making implant placement not favorable (Fig. 9).
These various views from this cone beam CT program allow the clinician to paint a picture of what the clinical post-extraction situation is and then be able to make decisions on the subsequent treatment steps. In this situation, grafting the ridge and allowing bone to form is what is called for to obtain the correct implant position for function and esthetics. Because of this information, Exactech’s Regenaform demineralized and mineralized donor bone putty (exac.com) was placed in the defects and allowed to heal for 6 months while the patient wore a denture.
The post-graft CBCT shows the cross-sectional and axial views of abundant bone growth (Fig. 10). The post-graft CBCT allowed for the creation of a surgical guide for implant placement in the ideal positions (Fig. 11). A surgical guide created from a CT allows for dental implants to be placed in the ideal position with regards to angulation, spacing and depth. After the dental implants were allowed to heal for 4 months, the BioHorizons abutments (biohorizons.com) were created (Fig. 12).
A post-completion panograph reveals dental implants in the ideal position to support a cement-retained fixed prosthesis (Fig. 13). In this case, the restoration came from da Vinci Dental Studios in West Hills, Calif. (davincismile.com). The final clinical photograph reveals much improvement over the original failing bridge in both esthetics and function (Fig. 14).
Conclusion
Part three of this article series on Cone Beam CT showed the importance of CBCT for planning esthetic cases and also for larger implant cases. The information obtained from the various views of a CBCT program offer substantially more information than a two-dimensional radiograph. Not only can spacing requirements be ascertained, but navigation around vital anatomical structures can be achieved. As a clinician uses these CBCT programs, an intuitive knowledge is had that has great clinical relevance. I hope this series of articles about CBCT has shown the clinician the importance of CBCT and how easily it can be used in daily practice.
RELATED Articles
- Make it pay: Dental implants
- A place at the table
















ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.

