How to treat facial pain with photobiomodulation/low-level laser therapy
How using photobiomodulation can help many patients with facial pain problems without the use of prescription medications.



Facial pain and TMJ disorders are problems that appear in our offices daily; sometimes we recognize it, other times we don’t ask the appropriate questions.
There have been numerous treatments proposed over the years: splints, biofeedback, occlusal equilibration, surgery, neuromuscular treatments, chiropractic, medications, and the list could go on and on. I have been treating facial pain on a referral basis for the past 38 years and have used many of these modalities.
There are numerous conditions associated with facial pain, but there is one common element in all these patients: pain. Early in my career, I used a lot of prescription medications to help these patients; pain medications, anti-inflammatories, tricyclic antidepressants to name a few. In 1993, I purchased my first low-level laser which resulted in me replacing the use of pharmaceuticals with a photobiomodulation (PBM) device.
What is PBM?
Unlike surgical lasers which utilize a photothermal reaction, PBM uses light to stimulate a cellular response.



Originally, PBM treatments were done primarily with lasers, but since then many of the devices now use LED cluster probes. There have been many terms used to describe these devices: low-level lasers, soft lasers, and cold lasers (Table 1). In 2012, a group of leaders in the field met and it was decided the universal term that would be accepted to describe this treatment would be photobiomodulation.
- Photo as it is light
- Bio as it elicits a biological response
- Modulation because depending on the dose, one can have either stimulation or inhibition.
Mechanism of action
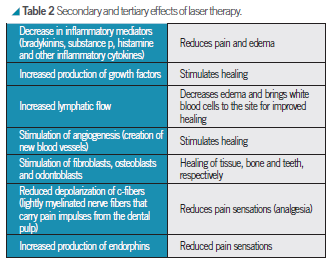
PBM works at the cellular level to stimulate the production of cellular energy in the form of adenosine triphosphate, or ATP. ATP can be thought of as the gasoline of the cell – it provides the energy needed to help a cell function and repair itself. Table 2 describes some of the secondary and tertiary effects of laser therapy.


The history of laser therapy
The use of light for healing and physical wellbeing is not a modern concept. For centuries, people have respected the healing nature of light and used it in different forms of clinical therapies. Hospitals frequently took patients to the rooftops to help improve patient’s health and light therapy has been studied and used for decades to combat winter depression or Seasonal Affective Disorder.
When studies on light began in earnest in the ’50s, many researchers were skeptical of the safety of light devices, often proposing any wavelength in the electromagnetic spectrum, similar to UV, would cause similar negative effects such as cancer. One such researcher, Dr. Endre Mester, set out to investigate whether this hypothesis was correct
and found that not only did the laser not cause cancer or cellular damage; it actually stimulated the healing of wounds and hair growth.
This was one of the first documented demonstrations of the biostimulatory effects of light. Since then, thousands of studies have been conducted on the use of laser therapy, which have been published in esteemed journals such as Nature, Pain, and The Lancet. Further, laser therapy has been included in several evidence-based clinical guidelines for neck pain, Achilles tendinitis, and rotator cuff injuries.
Safety
In the stimulation model, it is only cells that are deficient in or incapable of producing optimal amounts of ATP that will be affected by PBM. Once the optimal amount of ATP is being produced, our cells use the enzymes called ATPases to cease the ongoing production of cellular energy. As such, healthy cells will be unaffected by laser light and there are no detrimental side effects to PBM. This has been demonstrated repeatedly in literature and is why it is such an appealing treatment modality to an increasing number of healthcare professionals.
Using the appropriate dose
Treatment dose is probably the most important variable in laser treatment. Dose is measured in joules per square centimeter (J/cm²) and is a measure of the amount of energy that is conducted into the tissue. Clinicians should be aware of the optimal dose for each application to maximize the beneficial effects of laser therapy. The clinical effects of laser, such as wound healing, pain relief, or muscle relaxation, are all sensitive to different irradiances or doses.

Fig. 1 The biostimulatory and inhibitory effects of lasers are governed by the Arndt-Schultz Law.
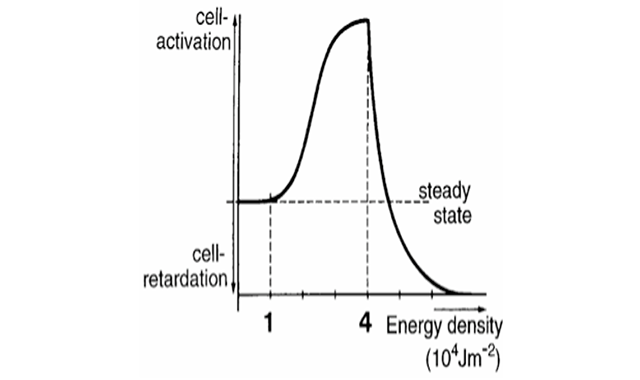
The biostimulatory and inhibitory effects of lasers are governed by the Arndt-Schultz Law (Fig. 1), which indicates that weak stimuli will increase physiological processes and a strong stimulus will abolish physiological activity.1,2
For applications where you are looking for biostimulation (e.g. stimulation of fibroblasts or osteoblasts for healing), use a lower dose. For applications where you are looking for bioinhibition (e.g. pain control), you want to use a higher dose.
In short, there is an optimal dose for each clinical application and one should be aware of this for ideal treatment outcomes.
PBM and facial pain
The first thing I want to stress is PBM treatment (PBMT) is one tool in my treatment of these conditions. I find greater success when I work with other health professionals; physiotherapists, chiropractors and, psychologists. What makes PBMT unique for pain control is that not only does it reduce the pain, but it also stimulates healing.
Secondly, the key to success using PBM is patient communication. Every patient reacts differently, so the key to success is listening to your patient and modifying the treatment according to their needs. PBM is patient communication. Every patient reacts differently, so the key to success is listening to your patient and modifying the treatment according to their needs.
The third key is something that I have learned from Dr. Jeffery Okeson:3
“Treat the source of the pain and not the site of the pain.” In other words, when applying the device, focus on treating the areas that are sore from your clinical muscle palpation and not where the patient says it hurts. Often
the pain in a muscle or joint refers pain to distant sites. This was documented well by Janet Travel in her classic textbook “Myofascial Pain and Dysfunction.” 4 The conditions I have found respond well to PBMT are Myopathic Pain:
- Degenerative Joint disease and TMJ osteoarthritis
- Pain in Joint and associated musculature in intracapsular problems
- Neuropathic pain and Trigeminal Neuralgia
As I stated above, one of the keys to treatment is to apply the laser to the areas that are sore to palpation. When I am treating, I use a laser with a 10 mm tip diameter in the smaller areas and a LED cluster probe over the larger muscles.
Among the areas I treat are:

Fig 2. In order to inhibit the system, the author uses a higher dose 8 J/cm2.

Large Intestine 4 (LI4) acupuncture point: In traditional acupuncture, this is one of the key points in treating upper body conditions. It balances the Yin and Yang as well as the sympathetic and parasympathetic nervous systems. It is great for reducing upper body pain. I want to inhibit the system, so I use a higher dose 8 J/cm2 (Fig. 2).
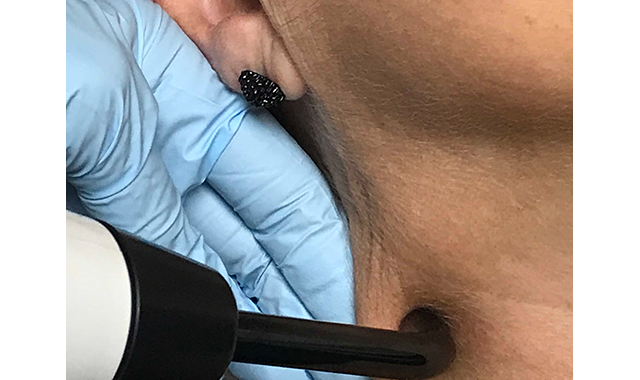
Submandibular Lymphatics: The lymphatic system is the body’s immune system and is very important in so many facets of facial pain treatment (Fig. 3). I want it to work more

Fig. 3 To work more efficiently, use a stimulation dose 4 J/cm2.

efficiently so I use a stimulation dose 4 J/cm2.
TMJ: In this area, I treat the joint with the teeth together and then have the patient open enough so the condyle translates and is out of the joint allowing me to treat the structures inside the joint more accurately (Fig. 4). It is pain control, so I want inhibition using a dose of 8 J/cm2.
Styloid area: This is the area behind the mandibular ramus that contains many structures vital to the operation of the jaw. When you palpate just under the ear in the styloid area you are palpating the joint capsule which is very highly innervated and is often very sensitive in intra-capsular joint problems.

Fig. 4 The patient opens enough so the condyle translates and is out of the joint allowing the treatment of the structures inside the joint more accurately.

As you continue down there is the Posterior Digastric Muscle, the TMJ ligament, and the stylopharyngeus muscle to name a few (Fig. 5). I find this often extremely sensitive to palpation. I am inhibiting pain so a dose of 8 J/cm2 should be used.

Fig. 5 The styloid area is the area behind the mandibular ramus that contains many structures vital to the operation of the jaw.

Lateral Pterygoid Muscle: This is the muscle associated with intracapsular joint problems, so I use an inhibition dose (Fig. 6).
Masseter Muscle: This is the muscle that is associated with clenching and bruxism. There are often trigger points in the muscle. If someone comes in with limited opening or locking, I find in most cases, the causes are muscle trismus within the Masseter muscle. I treat this muscle and in 95 percent of the cases there is a dramatic increase in opening, and I will proceed to treat them conservatively rather than send them off for a surgical consult.

Fig. 6 The author uses an inhibition dose on the lateral pterygoid muscle, which is associated with intracapsular joint problems.

Also, at the end of long appointments, many patients complain their jaw feels stiff so I will treat this muscle at the end of the appointment, so trismus does not set in (Fig. 7). It is a large muscle, so I use a cluster LED probe and use an inhibition dose.

Fig. 7 A cluster LED probe and an inhibition dose is used in the masseter muscle.

Temporalis Muscle: This is one of the two muscles I find associated with headaches. If the anterior or middle branches are tender, I often find this associated with occlusal slides or posterior working, balancing, or protrusive interferences. If the posterior branch is sore, it is often associated with bruxing. As a larger muscle, I use the clusters and an inhibition dose (Fig. 8).

Fig. 8 The temporalis muscle is one of the two muscles I find associated with headaches.

Sternocleidomastoid Muscle: This is the other muscle I find is associated with headaches. I often find trigger points in the body of the muscle (Fig. 9) or the mastoid area (Fig. 10) and use an inhibition dose.
Other dental PBMT applications: I find I am using my PBM units many times a day for many different applications. Some of these are:

Fig. 9 & 10 Locating trigger points in the body of the muscle or the mastoid area and using an inhibition dose can help combat headaches for patients.
- Pain reduction after extractions or surgery. In fact, PBM is so effective that I never prescribe opioids after even very compacted extractions and the patients experience very mild post-op pain
- Analgesia in teeth allowing me to complete many procedures without the use of local anaesthetic
- Treatment or prevention of soft tissue lesions: cold sores, aphthous ulcers, denture sores, and lichen planus
- Prevention and treatment of mucositis as a complication of chemotherapy or intraoral cancer radiation. In June of this year the MASCC/ISOO, the leading association of oncologists, accepted a report on the use of and safety of PBMT as a treatment of radiation/chemotherapy and it is now a recommended treatment to treat the most debilitating part of cancer treatment
- Nerve regeneration
- Aid in managing xerostomia
- Preventing nausea and gagging
PBMT in medicine
- There are a huge number of medical conditions where PBMT is being used or where research is being conducted.
- Among these are:
- Treatment of muscle pain, neck and back pain, and tendinopathies
- In athletics, almost all professional teams have PBM units to treat injuries. It has also been shown to improve performance
- Treatment of degenerative brain diseases. There is current research and studies being carried out using PBMT to slow Alzheimer’s disease, MS and Parkinson’s
- Treating dry macular degeneration
- Managing concussion side effects and cognitive problems associated with brain trauma
Conclusion
By using Photobiomodulation in my practice, I have been able to help so many patients with facial pain problems, and most importantly, I do it without the use of prescription medications. In the modern world, this is important to our patients, especially for the elderly who are often on a long list of medications when they arrive in our offices. In addition, PBM is invaluable to me. When I travel, I bring my personal unit. I never leave home without it.

































