Is your curing light 'bright' enough?
Why your curing light could lead to restoration failure.


You remember the procedure and know it went perfectly. Proximal margins clean and clear? Check. Proven high-quality composite and bonding materials? Check. Occlusion adjusted? Check. And yet a long-time patient sits in front of you with a prematurely failed restoration leaving you both asking “What went wrong?”
The truth is your seemingly trusty curing light may be letting you down far more often than you know. The familiar blue light may pop on when you press the button, but is sufficient energy actually being delivered to the composite?
Chris Felix is a materials scientist and noted author who has spent the last 16 years conducting research in the field of light-cured dental materials between Dalhousie University and BlueLight Analytics. Chris and I recently spoke in-depth about new technologies that address curing light performance issues.
As a researcher, you once supported manufacturers in developing better light-cured materials; however, the focus ultimately shifted. Talk about how your early research uncovered the significance of problems associated with curing lights and curing technique.
At the university, we provided highly accurate data on the interactions between lights and light-cured materials for some of the top companies in the world. It was relatively easy to show these manufacturers what light was better or what material had better properties under strictly controlled laboratory conditions.
But the oral environment is far from ideal laboratory conditions. To make our data more clinically relevant, we designed tests to simulate how light curing was done on a patient in a dental office. The first “aha moment” came from testing dental students and practicing clinicians under these clinical simulations to see how good they were at getting that light where it needed to go in the oral cavity. Some of them did really well, some did really poorly, but it was all left to chance. We uncovered a real gap in the dental training that existed because light curing was considered such a simple skill.
Trending article: IoMT and the future of dentistry
So, how frequently is poor curing light performance a potential culprit in restoration failure?
In the process of studying the interaction between various models of curing lights and light-cured dental materials, we amassed a huge database of more than 80,000 unique curing light tests. We were pretty astonished to find that at least one in five curing lights was significantly outside of the manufacturer’s specification. We define “significantly outside” as plus or minus 20 percent deviation from the stated irradiance, at which point there’s not much question as to whether the performance variation will have an impact on proper curing.
What determines whether a curing light is going to deliver the appropriate amount of energy to the materials?
Let’s presume the dentist is aware of and follows the manufacturer’s recommended settings and optimal curing times for each of the resins used in the practice. These recommended curing times assume the light is working to a specified output, or irradiance. Our data shows about 75 percent of the time that assumption is wrong.
One reason for this can be attributed to low-quality lights that are showing up in increasing numbers on the internet. We recently devised an automated test that cycles fully charged lights on and off until the batteries die and measures how the output varies over the charge cycle. While quality lights maintain nearly consistent output, we found some of these low-end lights were losing 50 to 60 percent over a single cycle - the worst one we tested lost 96 percent of its output. Based on this testing, I would advise dentists that reducing practice costs by purchasing cheap curing lights can be the single most expensive decision you make.



Even quality lights do degrade with normal wear and tear. Let’s say a light that had an original output of over 1,000 mW/cm2 drops to 800 mW/cm2 over two years of normal use. For some materials, a change of that magnitude might require doubling the curing time to achieve full polymerization.
Maintenance issues also can compromise curing light performance. Autoclaving tips have been shown to reduce throughput. If lights aren’t cleaned thoroughly, cured material can adhere to the tips, reducing the light delivered to restorations. Of course, the fiber optic tips can fracture or crack, so lights that are dropped should be tested before being returned to service.
Read more: Tips and tricks for creating long-lasting restorations
Please talk about new technology on the horizon that will help dentists detect these curing light problems before they impact patients
The simple dental radiometers available today are affordable but have reliability issues and limitations. Many radiometers only provide a simple pass/fail readout and don’t assist dentists with the interaction between their specific light with their specific materials. In our lab testing, we use highly accurate spectrometers. While spectrometers don’t have these limitations, they’re too fragile and expensive to be practical for dental practice.
As a solution, BlueLight Analytics has incorporated a cost-effective sensor technology driven by an advanced machine learning algorithm and a large database of spectral measurements to train this sensor to work as a virtual spectrometer. The database includes test results from a wide array of curing light makes and models as well as the recommended curing times from composite manufacturers.
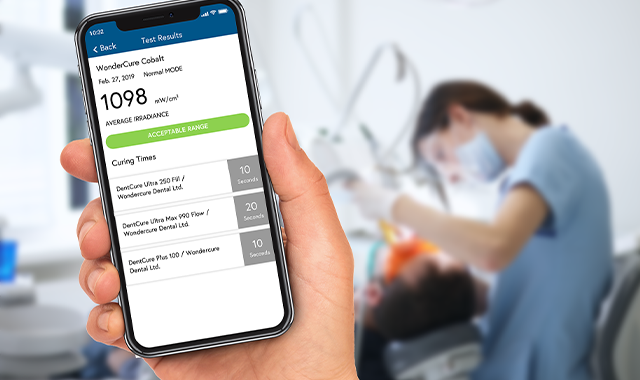
Via a smartphone app, the user gets the irradiance output of his or her light, recommendations in the case of malfunction and adjusted curing times for the specific materials used in that practice. The system, called checkUP, is currently in beta testing and should be commercially available in late spring.




























ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.

Product Bites – November 10, 2023
November 10th 2023The weekly new products podcast from Dental Products Report is back. With a quick look at all of the newest dental product launches, Product Bites makes sure you don't miss the next innovation for your practice. This week's Product Bites podcast features new launches from Amann Girrbach, DMG, Pac-Dent, and ASI Dental Specialties. [4 Minutes]



