Taking a look at strength and costs of leading bonding agents
An author and researcher tests several bonding agents and compares bond strengths and costs in an effort to help clinicians select which dental materials may be best for their practices.


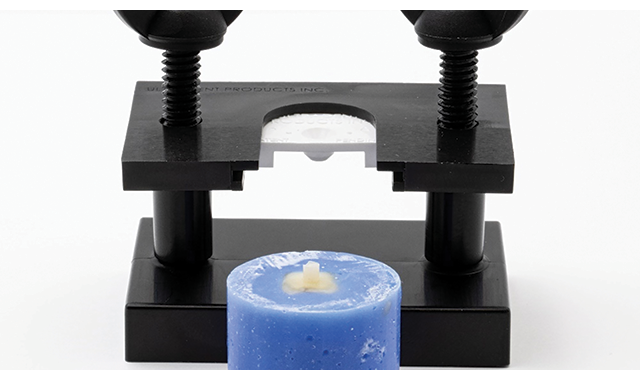
Figure 1. The test method used by Dr. Bess during his trials.
Information provided by Ultradent Products, Inc.
The average American Dentist is placing 8-10 bonded restorations daily. These are bonded to both dentin and enamel—when skillfully placed they can be indiscernible to the eye and provide years of service. Poorly placed restorations can fail before the patient reaches the parking lot. Every clinician is resting the success or failure of their practice—and reputation—on their ability to successfully bond to dentin and enamel, making bonding the backbone of modern practices. Selecting a bonding agent with the highest bond strength, along with mastering technique, can drastically reduce premature failures.
Navigating the crowded adhesives market to find the highest bond strengths can be frustrating. All manufacturers claim their products achieve “high bond strengths,” but what does that even mean? Strong compared to what? When they do give definitive numbers, manufacturers often compare three or four competing products with slightly lower numbers. Getting an actual number in expected bond strength in MegaPascals (MPa) out of some of them can take intensive investigation.
Testing
In 2019, I had uninhibited access to a $70,000 Instron machine and spent over 300 hours testing techniques and adhesives to see what achieves the highest bond strength of composite to both dentin and enamel. Not exactly how most people want to spend a year of their “free time”, but what I learned has changed the way I treat my patients. Not to mention I now have a lot to say to my dentist about bonding done in my mouth.
A lot of effort has gone into figuring out how to accurately test the strength of bonding agents between teeth and composite. To do this, we section human teeth and embed them in acrylic. Then we grind the surface with a disk to simulate fresh cut tooth structure. Once I had the specimens, I followed each manufacturer’s instruction in the application of their adhesive to either dentin or enamel. After the application of the adhesive and a 10-second cure with a VALO Grand curing light from Ultradent Products on the standard setting, I placed the specimen into a jig specifically designed to create a slow speed bur shank size of composite.
Careful packing of the composite into the opening was performed to achieve no bubbles between the tooth and composite. A 10-second cure of the composite with the VALO Grand, and then removal of the jig from the tooth was completed. A final 10-second cure at the same setting achieving the 20 seconds total cure time per instructions of the Z100 composite used was completed. All the specimens were then placed in a 37-degree Celsius (98 F) water bath for 24 hours. They were then placed individually into the Instron machine.
The Instron places controlled compressive force on the button of composite until it breaks. Upon breaking, the reading on the screen of the Instron Machine is in MPa. Because of the size of the composite button, MPa translates exactly into the pounds necessary to break. This brings MPa (not a unit that means much to most of us) into something that we can take out of the research world and use in everyday thinking.
Recording of each specimen was completed and averages of the bond strengths in MPa were recorded. Seven specimens of each bonding agent to dentin and seven specimens to enamel were obtained.


Results
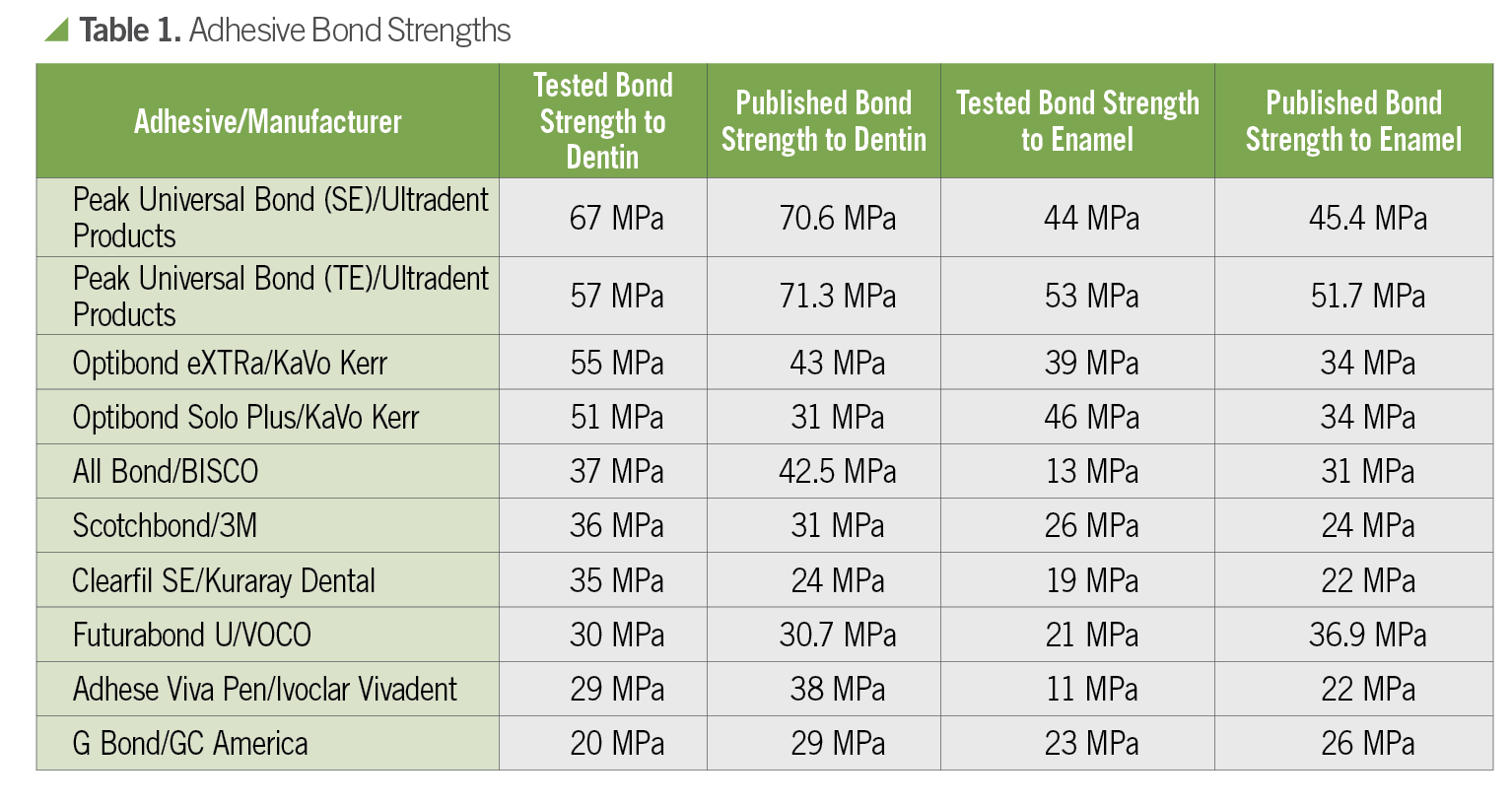
I discovered that bond strengths to dentin in the low 20’s are unfortunately all too common, and there are several bonding agents currently on the market scoring in the low teens when bonded to enamel.
When restoring an incisal edge with composite, or any restoration for that matter, the highest bond strength possible is what we dentists need. I fear many clinicians resort to full coverage crowns too quickly, based on experiences with an underperforming adhesive. They have no idea that the strengths of various bonding agents on the market vary so wildly. I recently attended a CE course at a well-respected university where one such dentist explained to the group that bonding small amounts of composite to mandibular incisors will not work. I know that particular clinician is not alone in his thinking.
Here you can see the results of some of the bonding agents I tested. The poorest performer to dentin had an average bond strength of 20 MPa. The poorest performer to enamel had an average bond strength of 11 MPa.
If you think of MPa as pounds of force applied to a slow speed shaft size button of composite bonded to tooth structure, you can appreciate the difference between 11 pounds of force required to break vs. 67 pounds. I can break 11 MPa (pound) buttons off with my thumb—I certainly can’t with 67 MPa. Perhaps the well-meaning dentist in my recent CE course is using one of these bottom dwelling adhesives.
Human dentin boasts a sheer strength of 70-90 MPa. Our Composite materials commonly have flexural strengths of 100-200 MPa and compressive strengths of 400-500 MPa. Why do we accept such low strength from our bonding agents?
Cost per ML
Bond strength is essential when evaluating adhesives but it’s not the only factor; cost is also critical. Comparing prices is a murky process with various kits for the different components. I used a refill bottle of adhesive, if possible, to get these numbers. I was genuinely trying to flesh out exactly how much the stuff costs per ML. I used the 2020 catalogs from Henry Schein and Ultradent, and the BISCO website.


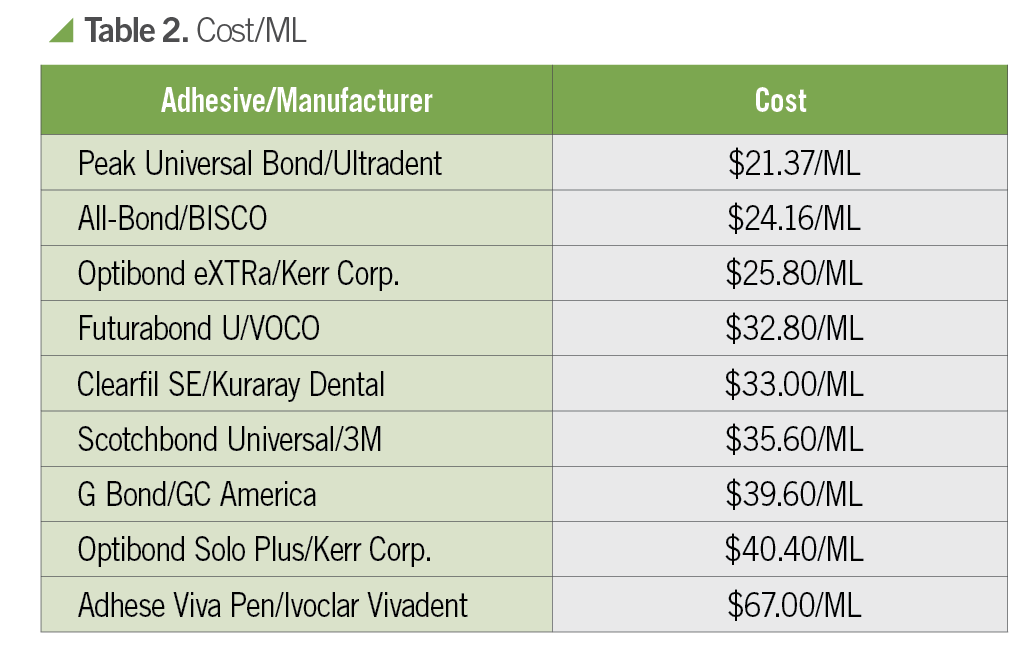
According to my research, Peak Universal Bond costs 40% less than Scotchbond Universal while providing nearly double the bond strength to dentin, and more than double the bond strength to enamel. Scotchbond Universal is the top seller in the United States.
I suggest every dentist find the strength of the bonding agent they use to both dentin and enamel. Get the actual numbers in MPa advertised by the manufacturer. Then compare to the top performers. Not just the two or three the manufacturer uses in their marketing. Then look at the cost per ML. Are you still happy with the bonding agent you use?
At this point, I can almost hear you saying, “Yeah, but what about sensitivity?” And this is a valid question. Sensitive restorations are a practice killer, and one of the many things that leads a practicing dentist to the medicine cabinet at night searching for an Ambien. Sensitivity is a serious concern, and something I believe has a lot more to do with the technique of the clinician than the product itself.
After more than 300 hours spent repeatedly testing adhesives, and 18 years of private practice, I have learned some very valuable lessons. Technique Matters! You must leave the dentin damp. As in, the ocean wave just went back out to sea, and the sand is saturated but doesn’t have any standing water on it, damp. If you overly dry the dentin, the adhesive cannot penetrate into the collapsed collagen. Want to avoid sensitivity? Do not desiccate dentin. There are several videos online that illustrate this nicely, and they are easy to find with a quick Google search.
I also learned most bonding agents want to be 12 microns thick. Think Saran Wrap thick. Once you have thinned the adhesive to Saran Wrap thickness, the solvent needs to be evaporated. Blowing air gently across it for 5-7 seconds will do this. A high-volume suction tip close by, drawing air across the tooth, will also get the job done quite nicely.
Contamination of the tooth surface with blood, saliva, water, or anything else will destroy your bonds. A high-quality curing light in the right place for the correct amount of time is critical.
Give all these things your undivided attention, and sensitivity will go to just about zero. Don’t believe me? I’ve been total etching dentin for many years now with extremely small numbers of patients complaining of sensitivity, and I’m not alone. If you are struggling with sensitivity, I would look first at technique. Follow the manufacturers’ directions exactly. Too many of us have never actually read how the manufacturer suggests we use their product.
Conclusion
I have talked with many clinicians who assure me they are not having problems with the bonding agent they use in their office. Perhaps they are correct. But, why use a more expensive product to obtain lower bond strengths? I admit that I used the bonding agent for years that they used in dental school. I was comfortable with it. Change can be hard and downright scary. But with costs rising, reimbursement not keeping pace, and the current economic situation, (thanks to COVID-19) finding ways to save money while improving performance is increasingly necessary.
Selecting a bonding agent with the highest strength and a lower cost could be your next step to improving your practice. Got courage?







 single fiberglass post system from Angelus.")























ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.

