Maximizing Value: The Hidden Benefits of Preventing Hospital-Acquired Pneumonia Through Oral Hygiene
Originally posted on Infection Control Today. Hospital-acquired pneumonia (HAP) is a significant infection prevention concern, leading to high patient mortality, increased health care costs, and ICU usage. Oral hygiene is an effective preventive measure.


Feature originally published in Infection Control Today. Glowing monitors in the intensive care department. Night shift at ICU, patient in a critical state. Image credit: © Adobe Stock 252813850 @ Kirl Lis

This article was originally published on Infection Control Today.
High Cost of Pneumonia
Hospital-acquired pneumonia (HAP) not only threatens patient safety but also exerts a significant financial burden on healthcare systems. According to the CDC's most recent point prevalence survey, HAP is the number one healthcare-acquired infection (HAI), accounting for one in every 4 infections.1 In addition to being highly prevalent, HAP impacts resource utilization, quality metrics, value-based purchasing (VBP) initiatives, and patient satisfaction.
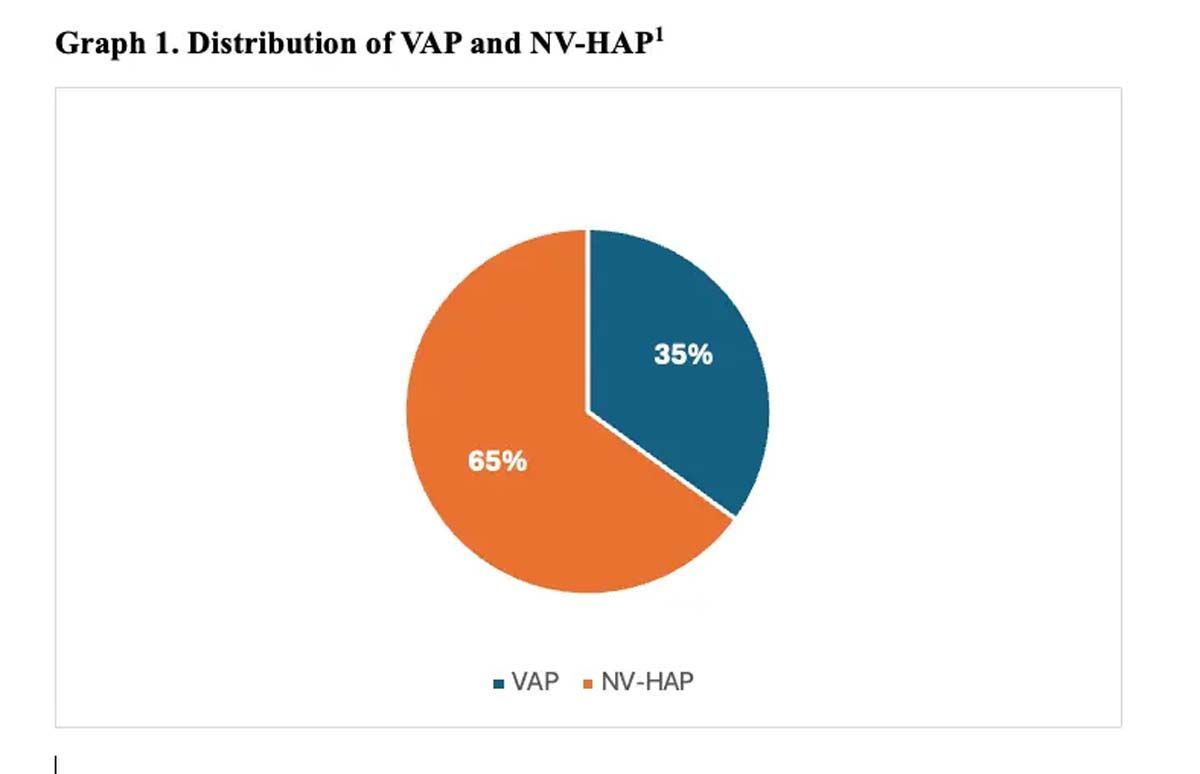
HAP is a confirmed pneumonia diagnosis that occurs 48 hours after hospitalization and is not present on admission.2 Ventilator-associated pneumonia (VAP) is associated with the use of an artificial airway, although most health care-acquired pneumonia (HAP) cases are not linked to a ventilator. Nonventilator-associated HAP (NV-HAP) is now a larger concern (Graph 1).

")
Table 1. Impact of Hospital-Acquired Pneumonia21-22
(Credit: Author)
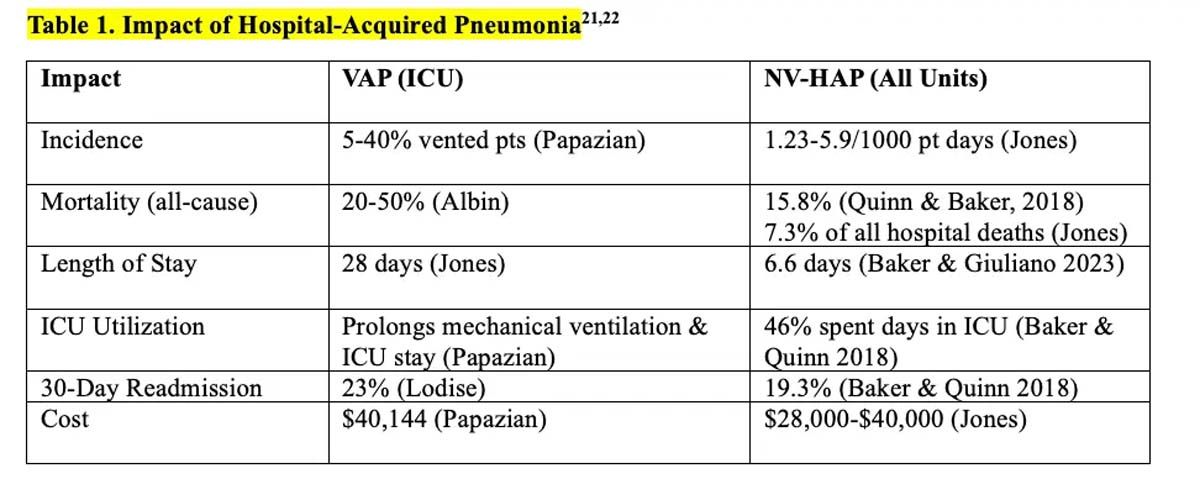
VAP and NV-HAP are frequent and serious preventable conditions that impact patients and healthcare systems. High mortality, increased length of hospital and intensive care unit (ICU) stays, increased utilization of ICUs, and frequent hospital readmission contribute to increased costs to patients, families, and institutions. (Table 1). In a retrospective case-control study of Medicare patients hospitalized in 2019, those with HAP were almost 3 times more likely to die within 90 days compared to matched controls without HAP, and those with HAP spent an extra week in the hospital, increasing the cost of care by 24%.3
Oral Hygiene as Prevention
While medical interventions are essential in managing HAP, oral hygiene's prevention role is often overlooked and is one of the most frequently missed elements of care.4 However, recent research underscores the hidden benefits of oral hygiene practices in averting VAP and NV-HAP, improving overall patient outcomes, including substantial cost savings and enhanced value-based care benefits.

")
Graph 1. Distribution of VAP and NV-HAP1
(Credit: Author)
Why use oral hygiene to prevent pneumonia? Oral hygiene is the only intervention that addresses source control by reducing the pathogens that lead to pneumonia. During hospitalization, the healthy oral microbiome is disrupted, allowing the growth and replication of pathogens that can cause infection.5 These pathogens are frequently microaspirated into the airway and can lead to pneumonia.6
Comprehensive oral hygiene breaks this chain of infection and combats pneumonia-causing pathogens before they can enter the lungs. Daily oral care is recognized as an Essential Practice in the pneumonia prevention guidelines updated in 2022.7 In a recent systematic review, daily toothbrushing was the most effective aspect of oral hygiene and was associated with a reduction in HAP, mortality, and length of stay.8
Multiple studies have shown a correlation between consistent oral hygiene and a reduction in HAP. One large urban hospital implemented a comprehensive oral hygiene program for all adult patients, including high-risk critical care and oncology. The 12-month study successfully increased oral care quality and frequency in all units and reduced NV-HAP by 39%, saving an estimated 8 lives, avoiding 500 hospital days, and saving $1.72 million in costs.9 As the implementation continued into another 12 months, oral care was incorporated into presurgical routines. Over 2 years, 164 NV-HAP cases were avoided, with an estimated 31 lives saved and $6.2 million in cost-avoidance.10

")
Table 2. Impact of HAP on Key Quality Metrics
(Credit: Author)

Cost Savings and Resource Utilization
Preventing HAP through an oral hygiene intervention yields tangible cost savings for healthcare institutions by sparing precious resources. HAP has a direct impact on resources such as ICU and hospital days and antibiotic use. HAP extends the length of time in the hospital. Patients must stay in the hospital for an additional 6.6 days for NV-HAP and 28 days for VAP.11,12
HAP drives ICU utilization from nonventilated ICU patients as well as patients on medical units. In a US 21-hospital study by Baker and Quinn (2018), 46% of patients with NV-HAP required critical care, and 27% were transferred to the ICU from medical and surgical units.13
HAP requires the use of antibiotics at a time when stewardship is imperative. An astounding 50-70% of antibiotic usage in ICUs is prescribed to treat HAP.14 A large hospital system demonstrated a reduction in broad-spectrum antibiotic use when lowering NV-HAP.15 By providing an oral care intervention and preventing HAP, hospitals can decrease the length of patient hospitalization, minimize the need for intensive care services, and curtail antibiotic usage, all of which contribute to freeing up resources and lower healthcare expenditures.
Quality Metrics and Value-Based Purchasing
In addition to sparing resources, preventing HAP through oral hygiene aligns with quality metrics and VBP initiatives in healthcare. VBP programs incentivize hospitals to deliver high-quality, cost-effective care by linking reimbursement to performance on various quality measures, including infection rates and patient outcomes.16
HAP contributes to quality measures that impact financial reimbursement, hospital accreditation, and public reputation (See Table 2). One important metric is SEP-1, a VBP measure that affects CMS reimbursement.16 SEP-1 is a 3-hour all-or-none bundle focused on early recognition and treatment. SEP-1 compliance has been challenging, with a rate of less than 50% in US hospitals.17
HAP is the most common site of infection for hospital-acquired sepsis and the leading cause of death among hospitalized patients.17 Focusing efforts on preventing HAP by providing oral hygiene can reduce the number of sepsis cases in the hospital and relieve the burden of adherence to time-sensitive treatment.
Enhanced Patient Satisfaction
Improving oral hygiene brings financial benefits and enhances patient satisfaction, which is a crucial aspect of healthcare.18 When patients are hospitalized, they expect proper oral hygiene, and research indicates that they notice when it is not provided.19 To improve the patient's experience and sense of control, it is advisable to provide education about the importance of oral hygiene during hospital stays and assist with daily oral hygiene tasks.20 Engaging patients in daily oral hygiene offers an opportunity to improve a key quality metric: patient satisfaction. (Table 2)
Conclusion
The benefits of preventing hospital-acquired pneumonia through oral hygiene go beyond cost savings. Prioritizing a standard oral hygiene program not only prevents the risk of HAP but also affects resource utilization, quality metrics, VBP initiatives, and patient satisfaction. Integrating oral hygiene protocols into routine infection prevention practices is essential for the well-being of hospitalized individuals and healthcare organizations.
References:
- Magill SS, O’Leary SJ, Janelle DL, et al. Changes in prevalence of healthcare-associated infections in U.S. hospitals. N Engl J Med. 2018;379(18):1732-1744. doi:10.1056/NEJMoa1801550
- . National Healthcare Safety Network (NHSN) patient safety component manual. Centers for Disease Control and Prevention. Chapter 6: Pneumonia. 2020;6-1 – 6-17.
- Baker DL, Giuliano KK, Desmarais M, et al. Impact of hospital-acquired pneumonia on the Medicare program. Infect Control Hosp Epidemiol. 2023;1-6.
- Mainz H, Tei R, Andersen KV, Lisby M, Gregersen M. Prevalence of missed nursing care and its association with work experience: A cross-sectional survey. Int J Nurs Stud Adv. 2024;6:100196.
- Kitsios GD, Morowitz MJ, Dickson RP, et al. Dysbiosis in the ICU: Microbiome science coming to the bedside. J Crit Care. 2017;38:84-91.
- Scannapieco FA, Giuliano KK, Baker D. Oral health status and the etiology and prevention of nonventilator hospital-associated pneumonia. Periodontol 2000. 2022;00:1-9.
- Klompas M, Branson R, Cawcutt K, et al. Strategies to prevent VAP, ventilator-associated events, and NV-HAP in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol. 2022;43:687-713.
- Ehrenzeller S, Klompas M. Association between daily toothbrushing and hospital-acquired pneumonia: A systematic review and meta-analysis. JAMA Intern Med. 2023;184(2):131-142.
- Quinn B, Baker DL, Cohen S, Stewart JL, Lima CA, Parise C. Basic nursing care to prevent nonventilator hospital-acquired pneumonia. J Nurs Scholarsh. 2014;46(1):11-19.
- Baker D, Quinn B, Ewan V, Giuliano KK. Sustaining quality improvement: Long-term reduction of nonventilator hospital-acquired pneumonia. J Nurs Care Qual. 2018;34(3):1-7.
- Baker DL, Giuliano KK, Desmarais M, et al. Impact of hospital-acquired pneumonia on the Medicare program. Infect Control Hosp Epidemiol. 2023;1-6.
- Jones BE, Sarvet AL, Ying J, et al. Incidence and outcomes of non-ventilator-associated hospital-acquired pneumonia in 284 US hospitals using electronic surveillance criteria. JAMA Netw Open. 2023;5
- Baker D, Quinn B. Hospital-acquired pneumonia prevention initiative-2: Incidence of nonventilator hospital-acquired pneumonia in the US. Am J Infect Control. 2018;46:2-7.
- Albin OR, Admon AJ. Accurately measuring preventable ventilator-associated pneumonia deaths using observational data: It’s about time. Ann Am Thorac Soc. 2021;18(5)
- Lacerna CC, Patey D, Block L, et al. A successful program preventing nonventilator hospital-acquired pneumonia in a large hospital system. Infect Control Hosp Epidemiol. 2020;1-6.
- The hospital value-based purchasing (VBP) program. Centers for Medicare & Medicaid Services. Updated February 6, 2024. Accessed May 25, 2024. https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/hospital-value-based-purchasing
- Barbash IJ, Davis B, Kahn JM. National performance on the Medicare SEP-1 sepsis quality measure. Crit Care Med. 2019;47(8):1026-1032.
- HCAHPS: Patient’s perspectives of care survey. Centers for Medicare & Medicaid Services (CMS). Updated September 6, 2023. Accessed May 26, 2024. https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/hospital-value-based-purchasing/hcahps
- Gustafsson N, Leino-Kilpi H, Prga I, et al. Missed care from the patient’s perspective: A scoping review. Patient Prefer Adherence. 2020;383-400.
- Murray J, Paunovic J, Hunter SC. More than a mouth to clean: Case studies of oral health care in an Australian hospital. Gerodontology. 2023;00:1-12.
- Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 2020;46:888-906.
- Lodise TP, Law A, Spilsbury-Cantalupo M, et al. Hospital readmissions and mortality among intubated and mechanically ventilated adult subjects with pneumonia due to gram-negative bacteria. Respir Care. 2021;6(5):742-750.















2 Commerce Drive
Cranbury, NJ 08512


All rights reserved.