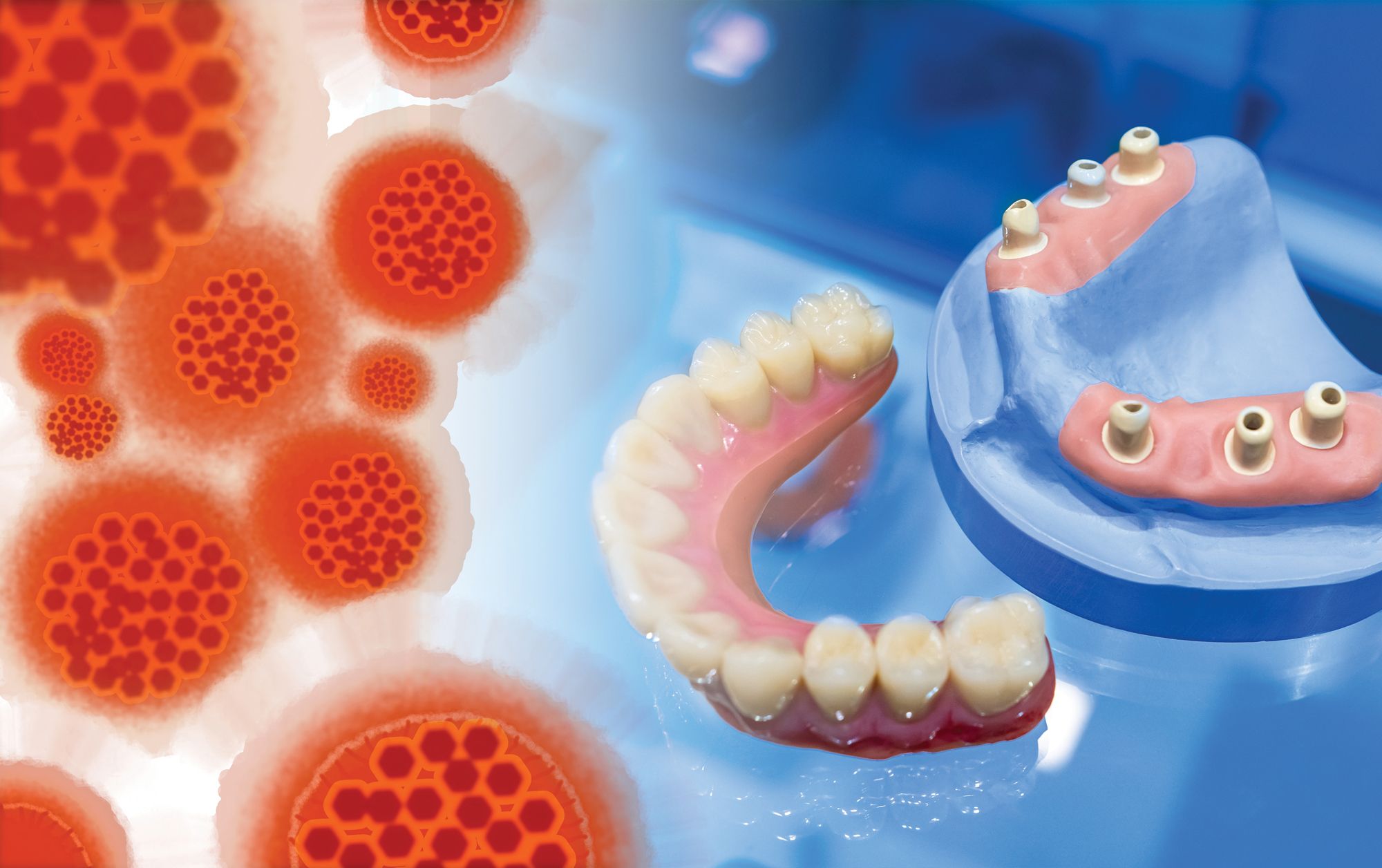
Infection Control for In-house Labs
In-house dental labs face unique infection control challenges every day. Here are some key insights for maintaining best practices for infection prevention in the in-house dental lab.


Infection Control for In-house Labs. Image courtesy of Grispb/ stock.adobe.com.
By all outward appearances, Mrs Johnson seems like a perfectly lovely person. When she arrives for her appointment, the twinkle in her eye, her sweet smile, and her charming demeanor covers her dangerous secret.
Once seated for her denture adjustment, the appliance is taken from her mouth into the back where staff start the adjustment. Unfortunately, some sloppy handling has led some of the bacteria on the denture to waft through the small lab area. The episode underscores the need for proper infection control protocols throughout the practice—not just in the clinical areas.
Scope
In-house dental labs come in different shapes and sizes. At its most basic, the lab can be a corner of a room to perform fundamental work, such as processing impressions or adjusting appliances. In some cases, the practice may have a full-size dental laboratory colocated on the premises.
“In the past, many dental practices combined what they would call their lab, where they have a model trimmer and equipment to pour up models, and a laboratory lathe, where they would polish temporary crowns or dentures. And they’d have it in the same area as the sterilization area,” Mary Govoni, CDA, RDH, MBA, infection prevention speaker, author, and consultant, says. “Some still do because of space limitations, but that is a big infection control issue. If you have sterile instruments also stored in that area but you’re doing activities like trimming and polishing, there is potential for cross-contamination. Ideally, those 2 functions should be separated, if not by a barrier, then in a different room.”
Digital Dentistry
CAD/CAM has changed the face of dentistry in the past 2 decades. Not only has it made lab work faster, easier, and more consistent, but it has also made the work safer. “A greater percentage of dental offices have intraoral scanners,” Jackie Dorst, RDH, BS, says. Dorst is an infection prevention consultant and speaker. “They scan the tooth and send that digital information to have a crown, bridge, or veneer created at a commercial laboratory. In the 1970s and the 1980s, they would take an impression of that tooth, [which] had to be physically shipped by postage or some other delivery service. You can imagine that impression coming out of a patient’s mouth where there is now gingival trauma and tooth preparation debris. There can be blood present or even some gingival tissue in the impression that has the risk for transmitting diseases from the dental office to the laboratory and to the technicians there. Nowadays, the dentist can do an intraoral scan and create a digital model [that] they can use to make a crown in their office while the patient is still in the chair. It reduces the risk of disease transmission within the laboratory,” Dorst says.
Safety First
No matter the size, safe practices must be observed to ensure proper infection control. “Let’s take the impression, for example,” Govoni says. “I’ve taken a preliminary alginate impression on a patient, and now I’m going to take it into the lab and pour up the model. The first thing I need to do is rinse all the saliva and any blood out of that impression, then I need to disinfect it. Now, if it’s a conventional alginate impression, I’m probably going to need to spray it with a disinfectant, wrap it in a moist paper towel to keep it from distorting or drying out, and let it sit for the necessary time [as directed by the manufacturer].
“If it’s a vinyl impression, then I can rinse it, get all the debris out, and I could immerse it in a container that has surface disinfectant in it, or again, I can spray it and let it sit for the required amount of time,” she says. “The advantage of using a vinyl material is that it’s not sensitive to drying out and distorting. If I’m going to polish a denture, I’m going to certainly take it out of the patient’s mouth, rinse it well, and disinfect it with a product that is compatible with the denture material. Everything I use when I’m working on that is going to need to be disinfected or disposed of after I’ve used it.”
The Right Way
Dorst refers to the Organization for Safety, Asepsis, and Prevention’s (OSAP’s) From Policy to Practice: OSAP’s Guide to the Centers for Disease Control and Prevention (CDC) Guidelines, which describes the 4 steps for safe in-house lab work. “Step 1 is when the impression comes into the laboratory,” Dorst says. “You’ve removed it from the patient’s mouth, then you want to rinse it under running tap water. That tap water should be at room temperature, not really hot or really cold. You can understand if it was really hot, it might affect the dimension, and those dimensions have to be very precise. Then, if there’s a lot of blood and saliva and debris in there, the assistant can use a soft camel hairbrush to remove the debris. [Being] gentle is important, so you don’t get what is referred to as dimensional distortion.”
Once the impression has been cleaned, it must be disinfected. “Step 2 is to disinfect the impression using an intermediate-level hospital disinfectant for the correct contact time,” she says. “That means you’re either going to spray it with the disinfectant or dip it in the disinfectant. But again, the dentist and dental assistant [must] review the manufacturer’s instructions for disinfecting that impression material, because it’s different between alginates, vinyl polysiloxane, and other common impression materials. After the manufacturer’s recommended contact time has elapsed, [step 3 says to] thoroughly rinse that impression under tap water to remove any of that chemical. Again, [use] room temperature or tepid water with it. After thoroughly rinsing, [step 4 says to] gently shake the impression material off. This is all done in the laboratory sink to minimize the spatter from it.”
Missteps
Where do practices slip up when it comes to in-house lab work and infection control? “One of the common mistakes I see is many practices fail to disinfect either the prosthesis or the impression before they send them out,” Govoni says. “According to CDC requirements, you must disinfect and/or sterilize anything that’s sent out of your practice. The laboratories typically do that as a redundant procedure, meaning they disinfect when they receive cases, because they don’t always know—or perhaps they don’t trust—that they’ve been disinfected before they left the practice.”
Like so many things in the dental practice, disinfection necessitates understanding the material being used and following the manufacturer’s specific instructions. “They can talk to the manufacturers of the impression materials they use if they’re sending out an impression,” Govoni says. “Then they can talk to their dental laboratory technicians to know what’s compatible with any kind of a prosthesis.”
Laboratory safety isn’t limited to lab work itself. “Another issue for [clinicians who] have a full-on fabrication laboratory is not necessarily related to infection prevention and control but to occupational health,” Govoni says. “It’s not having adequate ventilation, because there’s a lot of dust that is produced when items are fabricated. They need to have vacuums right at their workbench, and they should have good room ventilation to remove any of those dust particles from the air in that lab.”
Restorations going into a patient’s mouth aren’t the only things that are worth consideration. The restorations being removed also require handling with care. “The dental team may remove an appliance from a patient’s mouth, and it needs to be trimmed or modified in some way in the laboratory,” Dorst says. “I’m going to use a denture as an example: A denture’s been removed, they take it into the laboratory, and they don’t thoroughly clean it and disinfect it before working on it. [Now] all the lab equipment is contaminated and must be cleaned, disinfected, and sterilized or discarded. Not only is there surface biofilm and bacteria on that denture, but there could [also] be subsurface bacteria. If the laboratory technician or the in-office dental assistant doesn’t have on a mask and they’re using a bur or anything on that, [then] as that subsurface bacterium is released, they could potentially inhale it. Wearing full personal protective equipment [PPE]—a mask, safety glasses, gloves, and barrier gown—protects employees in the laboratory.”
Even some of the smaller tools need attention. “One of the big lapses I see is that they don’t clean and autoclave the acrylic burs and rag wheels,” Dorst says. “These items can be autoclaved. The best practice would be to use a new rag wheel for each 1 of those appliances, but I do see offices reusing those rag wheels.”
PPE
Appropriate PPE isn’t just the purview of the clinical areas. Those working in the lab areas must also ensure they are properly protected. “It’s very similar to the clinical area,” Govoni says. “Respiratory protection would be the biggest issue, especially for someone who is fabricating appliances or other types of devices. Again, even if they have that evacuation system right at their workbench, they still should be wearing an N95 respirator because of all the dust. Safety glasses or a face shield should be worn to prevent any particles from getting into the eyes. And when they initially handle something before it’s been disinfected, of course they need to be wearing gloves. Once it’s been disinfected, then it’s according to whatever their protocol is that they’re going to wear gloves while they’re fabricating. But most [clinicians] just simply wear the gloves all the time.”
Of course, PPE is very necessary, and it’s a great idea to ensure everybody gets adequate infection control training. “If a practice has its own lab and they have employees that work only in that lab, they [must] make sure they’ve had their Occupational Safety and Health Administration [OSHA] training, just like the rest of the clinical and administration team in a practice,” Govoni says. “They [must] understand all the principles of infection prevention and control, chemical safety, and all that. Make sure they are included in the OSHA training for the practice.”
Mrs Johnson isn’t a bad person. It’s not her fault that her dentures harbor dangerous pathogens, but ensuring proper lab safety protocols are followed can prevent those hazards from endangering others.


























ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.




