Imagining the Future: Dental Products We Wish We Had
In an industry that is always changing and improving, it can almost be hard to imagine how much better things can get. Here is a look at industry experts’ hopes for future products.


Imagining the Future: Dental Products We Wish We Had. Photo courtesy of stnazkul/stock.adobe.com.

Dentistry relies heavily on technology, and, by extension, technological advancements. These advancements are what makes the industry ever-changing and allows clinicians to deliver the best possible care to patients. Even in just the past 10 years, dentistry has come leaps and bounds in delivering innovations born from new technology that improves quality of life for both patient and practitioner. A wide range of products, such as more ergonomic chairs for the clinician and artificial intelligence-boosted scanning and treatment planning, are just some of the myriad ways dentistry has evolved over the past decade.
Despite how far we’ve come, there are still specific needs dental professionals have today. Technology advances more and more every day, and with each new insight, new techniques and products become possible. Building on these possibilities is what makes dental professionals best able to serve both themselves and their patients. With these insights, there must be a desire to improve and the effort to keep going. After all, if there is no effort to improve, there is no innovation. Without innovation, dentistry becomes stagnant and practitioners and patients suffer. Looking to the future, here is a wish list compiled from industry experts on what dental products, innovations, and techniques they are most hopeful for, for the future of dentistry.
Magnetic Resonance and Ultrasound for 3-D Imaging
[By Brooke Blicher, DMD ]
Cone beam computed tomography (CBCT) imaging has been a game changer in endodontics. Having the ability to 3 dimensionally visualize a tooth prior to initiating treatment has revolutionized the delivery of care, as have improvements in diagnostic accuracy and the detection of anomalies, such as resorption and fractures, that can greatly affect treatment planning.
On the other hand, CBCT technology exposes patients to higher doses of ionizing radiation than traditional radiography, so these benefits must be carefully weighed against risks. Therefore, I am most excited by the prospect of nonionizing imaging modalities under investigation for dental applications, including MRI and ultrasound.1-3 Both allow for 3-D imaging, thus maintaining the benefits and applications currently employed by CBCT without 1 iota of radiation exposure.4 As a result, the principle of maintaining exposures as low as reasonably achievable germane to radiographic imaging loses relevance, making imaging safer and more accessible to pediatric populations and potentially broadening applications.
Clinicians might use nonionizing 3-D imaging to track the progress of access and instrumentation of canal spaces in real time, which is an especially useful concept in the treatment of calcified teeth. Additional intratreatment applications include accurate and immediate working length determination. Close interval follow-ups without concern of unnecessary exposures would allow for early and frequent monitoring for healing pathology. As MRI images generally have better contrast and are less prone to scatter artifacts secondary to restorative materials, they may be especially well adapted for the detection of fractures and notoriously difficult to diagnose, even with high resolution CBCT imaging modalities.4 Additionally, MRI is able to accurately image both hard and soft tissues, including in the detection and mapping of decay and periapical pathology and the assessment of vitality and vascularity of pulp tissues. In particular, ultrasound has been shown to accurately trace sinus tracts of endodontic origin, although it remains to be seen whether it could have broader dental applications.
Ultimately, this technology remains a few years off from clinical practice. Although MRI and ultrasound are germane in the visualization of soft tissue structures and pathologies in the medical fields, the technology must be scaled and refined to suit the oral cavity and dentistry. Its introduction will undoubtedly allow for greater accuracy and understanding of dental anatomy, with obvious benefits for the clinician and patient. I look forward to someday incorporating nonionizing imaging modalities to improve the delivery of endodontic care.
References
1. Cotti E, Musu D, Goddi A, Dettori C, Campisi G, Shemesh H. Ultrasound examination to visualize and trace sinus tracts of endodontic origin. J Endod. 2019;45(10):1184-1191. doi:10.1016/j.joen.2019.07.009
2. Di Nardo D, Gambarini G, Capuani S, Testarelli L. Nuclear magnetic resonance imaging in endodontics: a review. J Endod. 2018;44(4):536-542. doi:10.1016/j.joen.2018.01.001
3. Idiyatullin D, Corum C, Moeller S, Prasad HS, Garwood M, Nixdorf DR. Dental magnetic resonance imaging: making the invisible visible. J Endod. 2011;37(6):745-752. doi:10.1016/j.joen.2011.02.022
4. Schuurmans TJ, Nixdorf DR, Idiyatullin DS, et al. Accuracy and reliability of root crack and fracture detection in teeth using magnetic resonance imaging. J Endod. 2019;45(6):750-755.e2. doi:10.1016/j.joen.2019.03.008
A Patient Education Tool That Shows Biofilm
[By Lynne Slim, RDH ]
I would like to convince a company to create a patient education tool that shows the growth of an oral biofilm on a tooth/root. I see it being presented from a mobile device app, TV education, or even a simple YouTube presentation. Hygienists often use their cell phones or operatory tablets to educate patients. Years ago, clinicians used to motivate patients to remove dental plaque by offering some dental plaque on a cracker (I know—gross!).
For several decades, some clinicians would take dental plaque samples and put them under a phase contrast microscope. After doing this for approximately 5 years, I can tell you that motivating my patients to improve their oral hygiene was easy after I showed them the various microbes under the microscope. I credit Paul Keyes, DDS, and his nonsurgical treatment approach to the management of chronic periodontitis for motivating me and others to step up our oral hygiene education efforts. Sandy Sheffler, RDH, and Sheila Wolf, RDH, (also known as Mama Gums from mamagums.com) are still promoting phase-contrast microscopy and both are very talented at motivating patients.
Now that science has taught us that periodontal inflammation appears to be the result of an interaction of the host immune system to subgingival biofilm, isn’t it time to get excited about visual displays of oral biofilm? I initially saw a 3D presentation of growing biofilm online that was part of an e-book from the Center for Biofilm Engineering at Montana State University.
Like phase-contrast microscopy, the message would be simple but powerful: Oral biofilm grows and changes above and below the gumline. From there, clinicians could elaborate about host inflammatory response.
Utilizing Pediatric Teeth Appliances to Track For Safety
[By Shannon Pace Brinker, CDA]
As a mother of 6 and a grandmother to 9 children, if someone were to ask me what my biggest fear is, my answer would be child abduction. Eight million children are reported missing each year worldwide, with an estimated 23,000 children being reported missing daily in the US. In 2020, there were 178,747 male juvenile kidnapping cases and 290,375 reported cases of abducted girls. Statistically, the first 3 hours after a child is abducted are the most critical to finding the child. Seventy-four percent of abducted victims are killed within the first 3 hours.1
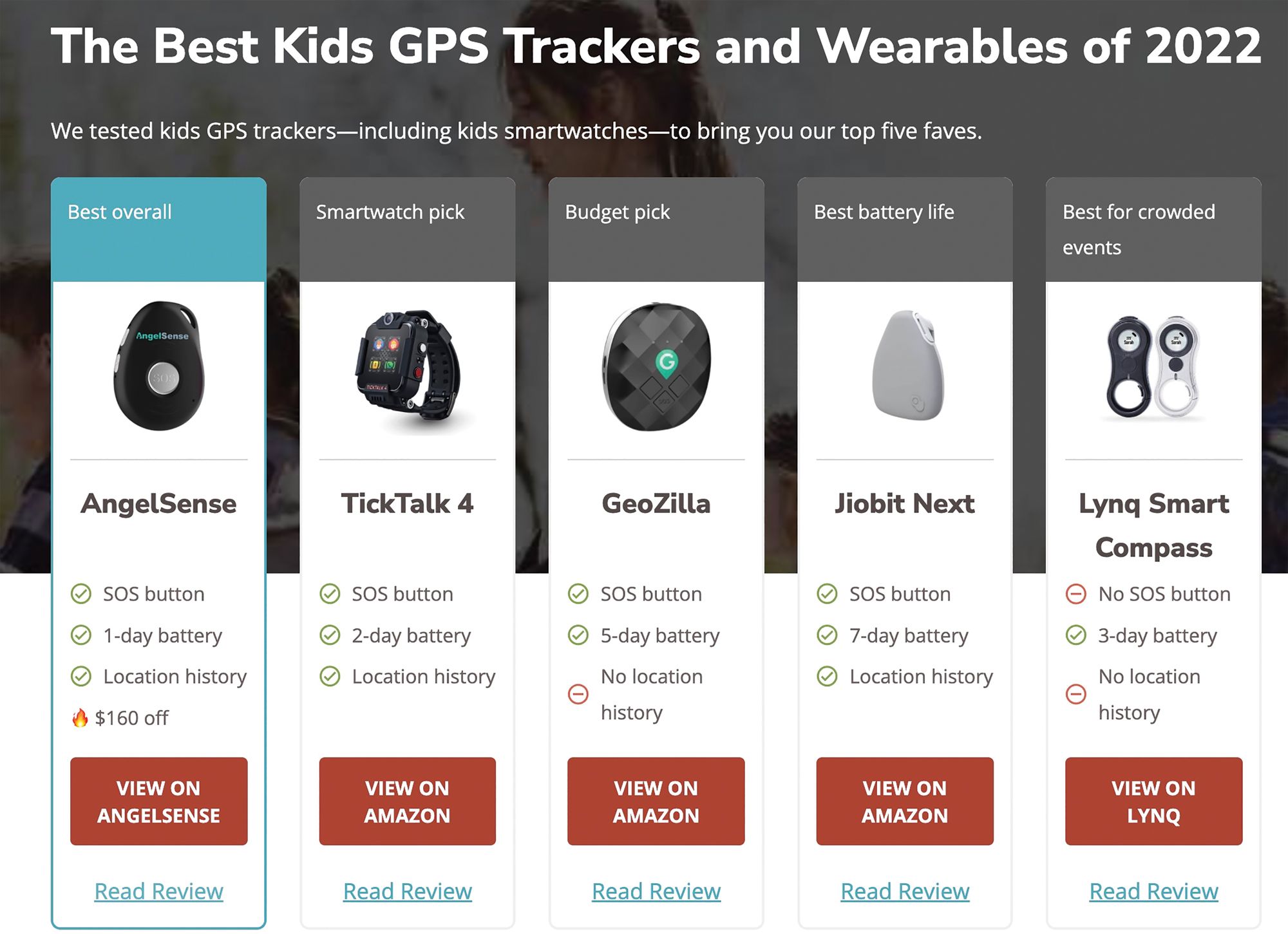
As a result, many feel that having a GPS tracker is the best way to track our children. There are several options on the market today, but most of these either lock tight into a school bag, clip onto clothing, or are a built-in smart watch. All these options have 2-way calling functions but have monthly fees attached.
Few children have fingerprints taken and many do not have dental records. One fantastic product that was developed many years ago as a simple, cost-effective way to provide a unique record of the child was a wax wafer impression that registered the shape of the patient’s teeth and overall bite. After softening the wax wafer impression, it is then sealed in a plastic bag and given to the patient’s parents to keep in a safe place at home. The tooth print system provides dental identification and supplies DNA sources from the saliva proteins on the wafer. Saliva can also make way for an effective tool for scent tracking with dogs. But let’s be honest, this is for identification.


There are a variety of different GPS tools that parents and guardians can utitlize to keep their children safe. In the future, there could come a time when pediatric teeth appliances can do this job safely and effectively without causing any major disruption to the child’s quality of life.
I feel this is a good product that we should continue to utilize in our practice, but no one knows about it. This product would also require seeing the patient to take this valuable record. There are other options for keeping our little ones safe by utilizing a GPS tracker, such as an app that gives frequent updates and has virtual capabilities to track your child’s location. However, if it’s forgotten, not charged, not tracked, or not compatible with all cellular networks, then what good does it do?
With artificial intelligence, robotic process automation, intelligent applications, and quantum computing machinery, why are we not thinking brighter? A microchip is a radio frequency identification transponder that carries a unique identification number and is approximately the size of a grain of rice. It can be scanned with a digital scanner to transmit the ID number. There is no battery, no power required, and no moving parts. As a result, a restoration placed just as easy as a dental sealant could save many lives. In primary or permanent teeth, I would do it for my kids. And when I asked my children whether they would use a product like this for my grandchildren, both moms agreed they would be first in line.
Reference
1. 23 alarming child abduction statistics 2021. Safe at Last. Published October 15, 2021. Accessed February 15, 2022. https://safeatlast.co/blog/child-abduction-statistics/#gref.
Chairside Checkout With Mobile Pay
[By Ryan Hungate, DDS, MS ]
Innovative Idea
Make it easier for patients to pay by adding wireless chairside checkout, mobile pay, and text-to-pay options.
Description
Smart phones have changed the way people shop. More than 100 million Americans use mobile pay for everything from point-of-sale purchases at Starbucks to riding the subway in New York City.1 Dental practices who still require patients to pull out a credit card or debit card—or worse, pay a bill by check—need to change to a payment processor that makes it easier for patients to pay the way they want.2
Companies like Simplifeye offer wireless card readers and accept Apple Pay, Google Pay, automated clearing house, credit cards, and debit cards, with tap-to-pay technology to enable chairside checkout. They also enable text-to-pay invoices, which is a must-have. A new study by Reviews.org discovered that 70% of Americans check their phones within 5 minutes of receiving a notification.3 By embedding a click-to-pay link, companies get paid faster.
How quickly does the change need to happen? Consider this: In the first year of the pandemic, in-store mobile payments grew by 29% as grocery stores, convenience stores, and pharmacies started offering contactless payment methods. Now it’s become mainstream, with almost 70% of retailers accepting some form of contactless payment. Research firm eMarketer predicts more than half of all smart phone users will pay for goods and services with their phones by 2025.
So, what exactly is mobile pay? It’s when a person links their payment information to an app on their phone. Apple Pay, Google Pay, and PayPal are all examples of mobile wallets. They are smart phone apps where people can load their credit card or debit card credentials and use their phone rather than the physical card to make a payment. People of all ages enjoy the convenience. Millennials account for 40% of mobile wallet users—and by the way, millennials are now in their 30s and 40s.
References
1. Perez S. Fueled by pandemic, contactless mobile payments to surpass half of all smartphone users in US by 2025. TechCrunch+. Published April 5, 2021. Accessed February 11, 2022. https://techcrunch.com/2021/04/05/fueled-by-pandemic-contactless-mobile-payments-to-surpass-half-of-all-smartphone-users-in-u-s-by-2025/
2. Stern J. Wallets are over. Your phone is your everything now. Wall Street Journal. Published September 5, 2021. Accessed February 11, 2022. https://www.wsj.com/articles/wallets-are-over-your-phone-is-your-everything-now-11630846800
3. Wheelwright T. 2022 cell phone usage statistics: how obsessed are we? Reviews.org. Published January 24, 2022. Accessed February 11, 2022. https://www.reviews.org/mobile/cell-phone-addiction/
A Plumber’s Tape Optimized for Dental
[By Andrew E. Skasko, DDS]
If your go-to material for sealing the access channel of screw-retained implant restorations is found in the plumbing section of your local hardware store, it may be a sign that an upgrade is in order. I’ve gone as far as hiring my own CAD designer and carving up my curettes to create instruments that make packing and removing barrier material easier. Our profession and our patients deserve something better.
In reality, none of the traditional materials for managing implant restoration screw access chambers are ideal. Cotton pellets absorb moisture and disintegrate, making them hard to access and remove if maintenance is required. Over time, cotton also discolors and can facilitate microbial growth in the channel. A newer option I use primarily with temporization is elastic silicon. Although silicon is better than cotton, it can rip. If you have endured a fishing expedition to retrieve barrier material lodged apically, you know how time-consuming and challenging that can be.
Finally, there’s the popular hack of using polytetrafluoroethylene (PTFE) plumber’s tape. PTFE offers many desirable properties as a barrier material. It’s inert, moisture resistant, reasonably packable, and retrievable. Setting aside for a moment that plumber’s tape is not a medical product, its physical characteristics are not optimized for this sensitive dental procedure. As a flat ribbon going into a deep, round, and narrow hole, it requires tearing, twisting, and packing multiple pieces per restoration. This can be time-consuming and laborious. Additionally, a good barrier material should provide sufficient compressive force to minimize the possibility of the screw working itself loose. Although plumber’s tape is condensable, it doesn’t maintain the compression profile to best serve this function.
Most importantly, PTFE tape from the bin in your local hardware store is an industrial product. It may have nonbiocompatible additives and residuals from the manufacturing process, including lubricants, biocontaminants, and toxic dyes. Because it is manufactured in foreign factories without medical-grade protocols, you simply can’t know what you’re putting in your patient’s mouth with industrial PTFE tape.


Polytetrafluoroethylene plumber’s tape maintains qualities such as moisture resistance that any dental professional would desire in a barrier material.

The barrier material I want would have many of the desirable characteristics of PTFE plumber’s tape. It would be inert, moisture resistant, and packable. Its compression profile would be optimized to hold the retention screw securely in place. It would be easily accessible and retrievable for maintenance. From a design perspective, the ideal solution would be cylindrical to fit screw retention channels without manipulation, and it would be efficient to measure, dispense, and cut to the optimal length. It would come with custom instruments for fast and easy plugging, packing, and retrieval. Finally, it would have to be a biocompatible product made under medical-grade conditions. That’s the barrier material I’ve wished I had for years.
And sometimes wishes are granted. Late this past year, I learned about FirstPlug, a new medical-grade PTFE barrier material. It came with a wonderful set of instruments, including a plugger and excavator optimized for use with the FirstPlug material. The handling and performance are ideally suited for the purpose. Most importantly, FirstPlug provides the confidence we’re treating with a biocompatible medical-grade product consistent with the highest standard of care.
An AI-Assisted Full Digital Workflow
[By Jeff Lineberry, DDS]
There is no doubt that technology, like everything else, has impacted dentistry in ways we could not have even imagined 20 years ago. As technology continues to make inroads in our everyday living, it will continue to evolve and change how we practice dentistry.
The technology will lead us to a place where we can see things that change almost completely from how we are doing things currently. In fact, it is safe to say we are now entering a place where we will see changes in a logarithmic proportion, so hold on!
It would begin with having a digital intraoral scanner that can capture the absolute details of the oral cavity, teeth, and preparations without retraction as well as without the concern of moisture and other contaminates. A scanner that not only allows us to capture soft tissue accurately for a tissue-supported prosthesis but also captures margins on a tooth preparation that are subgingival and/or where moisture, blood, or contaminates prevent current scanners from working.
Today, digital intraoral scanners are becoming affordable and very accurate, but the need for tissue retraction and tissue management is still critical for overall restorative success and outcomes. In fact, sometimes the analog way of taking impressions allows us to displace tissue and offers better records vs digital.
My hope is that these technologies will lead dentistry into a paradigm shift, where things will become easier clinically and technically than it is now and be intuitive. I would love to see the overall digital workflow become artificial intelligence (AI) driven, allowing the time needed to process information, design, and recreate necessary outcomes reduced significantly.
In addition, we would be able to scan the face digitally, then be able to connect the data from our intraoral scans directly to 3-D CBCT scans. This can allow us to have a real and unique setup vs an arbitrary setup that is often used nowadays.
Many of these things are already available to us as a profession, but it requires time and auxiliaries to complete these tasks, not including added cost. Maybe one day we can have a software or an ability for all this information to be simply dumped into 1 place, where it would then get organized and recreate the data input to a point where we can simply look at the patient in their entirety. Then we could design and create treatment plans, direct the technology for the desired outcome, and easily share it with the patient and/or specialist.
All of this is not far-fetched from the current world as we continue to see technology change everything around us and we see the advent of AI impacting our lives right before our eyes. It is happening everywhere from our phones automatically correcting our poor spelling to programs that are intuitively finishing our sentences to searching the web for certain products, then having all the choices in front of us. Going forward, the key to all of this is making it readily available and affordable for all.
Using AI-Integrated Cloud Software to Boost Performance
[By Glenn Vo, DDS]
Artificial intelligence (AI) is up-and-coming in dentistry, and it’s revolutionizing the industry as we know it. One way AI is being adopted into dentistry is as a “dental assistant” that analyzes images and identifies abnormalities based off pretrained algorithms. Rather than replacing our role as dentists, it’s designed to provide a second opinion and help us make a more accurate diagnosis.
Once AI is integrated into cloud-based dental imaging software, such as SOTA Cloud or other cloud software, the entire dental experience is going to become seamless. AI integration into cloud software allows all patient information to be automatically uploaded into a centralized database. This will make it extremely easy for dentists and their staff to access patient information from various locations and provide evidence to back up their diagnoses.
When people ask why they should switch to a cloud practice management software or imaging software, I tell them to look at what’s going on in the world. Everything around us regarding storage is already moving toward cloud. For example, the pictures on your iPhone automatically get saved into iCloud. So why wouldn’t we do it in dentistry? It just makes things more efficient and much safer. If something happens to your server, then you’re at the mercy of whatever your information technology guy can do. When it’s in the cloud, you don’t have to worry about losing critical information because there’s so much support readily available.
I believe AI integration into cloud software will truly be a game changer for the industry. Although using AI to help with diagnoses is something new, I’m all for something that can help dentists provide better care for patients. It not only makes the job of the dentist easier, but it also allows for a higher level of performance.
AI integration into cloud software can analyze images more precisely than the human eye, eliminate bias, and display that information in a safe and efficient way. Ultimately, this will provide dentists with the support they need to make more informed decisions.
Much like any new technology, a bit of resistance to AI and its integration into cloud software can be expected. However, moving into the future, dental professionals should see these innovations are designed to save time, be more cost effective, and make our jobs easier to improve the standard of dental care.
A Truly Monolithic Printed Denture
[By Eric D. Kukucka, DD]
With the increased growth and awareness of digital removable prosthodontic treatments being seen globally, the advancements in materials, processes, procedures, workflows, and technology have grown at an exponential rate. As we know, one of the most challenging rehabilitations to provide in dentistry is removable prosthodontics. Digital technology has improved so many aspects of how we treat patients today without ignoring the importance of clinical fundamentals, knowledge, understanding, and research-based dentistry.
When we look at the evolution of dental materials, manufacturing methodologies can be simplified into 2 categories: subtractive and additive manufacturing, most commonly referred to as milling and printing. In the infancy stages of digital removable prosthodontic treatments, subtractive manufacturing was the industry standard and baseline of this treatment modality. As technology continued to innovate and materials evolved, additive manufacturing became implemented as part of these treatments, albeit in some instances only as auxiliary devices and interim restorations. Today we are seeing significant breakthroughs with respect to the physical properties of these materials as well as the rate at which these materials can be manufactured.
In my practice, I am still a proponent of subtractive manufacturing of polymethyl methacrylate (PMMA) materials for most of my definitive removable prosthetics, particularly the Ivotion monolithic Digital Denture Disc. This disc is a bicolored single disc that is manufactured in 1 uninterrupted milling process, producing a quality PMMA restoration in 1 manufacturing cycle. Subtractive manufacturing is also still a part of our daily practice manufacturing models, surgical guides, try-in dentures, and interim immediate dentures.
In light of the above, what I feel is needed and the product I wish we had would be the ability to print a denture base and denture teeth in 1 uninterrupted cycle, resulting in a truly monolithic printed denture. This would not only provide increased strength to the restoration but also improve the manufacturing process immensely.
It has been so gratifying to see the advancements in digital technology with respect to removable prosthodontics today, and I cannot wait to see what the future brings to the way we can rehabilitate edentulous patients and improve their quality of life.
A Mobile X-Ray Application for Patients Using Teledentistry
[By Alicia Dieujuste ]
Dentistry has come so far since I first started in the field 20 years ago. To give some context, we weren’t even using texting back then! There are so many amazing tools out there for offices to adopt. One area with immense opportunities is streamlining digital diagnoses.
The COVID-19 pandemic showed us how quickly things can change. Having teledentistry during that time allowed dental practices to see and speak with patients to diagnose oral issues but did not provide all the diagnostic information dentists are accustomed to. One diagnostic tool you cannot get via a video call or telephone is an x-ray of what is happening inside the patient’s mouth.
My dream for the future of dentistry is a secure mobile application that allows patients to take their own digital images and x-rays. Patients would download an application and use a disposable sensor with their own device, without leaving the house. This would enable more patients to receive assistance during a lockdown scenario, such as the one inflicted by COVID-19. It would also expedite care for patients who are bedridden or others who cannot easily make their way to a dental office.
Alternatively, SmileDirectClub has pioneered the concept of taking dentistry out of the dental office by creating walk-in offices in shopping malls across the country. In their model, they capture orthodontic impressions by scheduled appointments or walk-ins, without the patient having to visit a dental office. This provides greater access to treatment that otherwise may feel intimidating and resolves issues related to office hours by providing later hours to accommodate more patients.
I’d like to see a similar approach with other diagnostic tools like x-ray images, such as panoramic x-rays, cone beam computed tomography, and intraoral photos and impressions, which would enable patients to complete walk-in appointments. Taking this approach to dentistry could be the next step in removing barriers patients have, such as fear, time constraints, and accessibility. For patients who are dental-phobic, not knowing what their upcoming appointment may bring can be a roadblock to receiving care. Easing patients into dentistry with just an x-ray and a diagnosis before they commit to walking in the door for treatment will go a long way toward overall patient care.
Additional Milling Materials With a Range of Unique Properties
[ By Eric Mayuga, DDS]
My first adventure with chairside milling solutions began in 2004 with CEREC. I utilized the technology extensively for several years, then took a break to explore the wide array of new materials available through traditional dental laboratories, as chairside milling solutions were limited at the time. I wanted to ensure my patients were receiving the best restorations with optimal strength, esthetics, and quality. I returned to chairside milling with the Carestream by AG Manufacturing just before COVID-19 hit, without success. I decided to switch in early 2021, and after extensively researching the market, I purchased Roland DG’s DGSHAPE DWX-42W chairside milling solution. My ultimate deciding factor in purchasing the DWX-42W was that it was a solid, reliable chairside milling solution built by a great company with a long history of technological innovation in this space.
My patients are thrilled they can have a high-quality, durable restoration placed all in 1 appointment. It eliminates patient and staff anxiety that a temporary could possibly come off over the weekend or holiday. In addition, postoperative sensitivity is greatly reduced, and patients are happy they do not need a second appointment and possible additional anesthetic to cement the final restoration.
With the DWX-42W’s speed and ease of use, I can now offer inlays and onlays for patients and place more conservative restorations to preserve natural tooth structure. I currently use the Straumann n!ce block for all my restorations, and it polishes beautifully, with a precise fit and margins.
Another advantage of chairside milling is that insurance claim turnaround is much faster. Most insurance companies require the definitive restoration to be permanently seated before the claim can be sent. In the past, we would have to wait for 2 to 3 weeks while the crown is fabricated in a lab and returned to seat at another appointment. With the DWX-42W, we can send out a claim the same day.


Roland DG’s DGSHAPE DWX-42W’s quick milling time combined with the possibility of fast, high-quality scans in the future, holds the promise of a quicker chairside turnaround for happier patients.

Our office is growing, and we plan to add another dentist to our practice soon. I would like to have a second mill so the second clinician can offer the same excellent chairside service for patients. Currently, I only mill and place single unit restorations in the posterior region and have not explored anterior veneers or crowns, which I would like to add to our services. I would also like to explore restoring implants, along with milling multiple units and bridges.
In the future, I’d like to see additional materials with a range of properties come to market. For example, I would like to see a presintered zirconia block that can be milled in a reasonable amount of time. This may be already available, but I would like the ability to scan the tooth before preparation and mill a replica of the tooth so the patient feels the normal, natural contour they are used to.




























ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.




