How to use liner for pulpal protection in restorative dentistry
Lining dental material is frequently used beneath dental restorations to reduce the potential for post-operative sensitivity, but take on a much greater role long-term in serving as pulpal protectants.



Liners are frequently used beneath dental restorations to reduce the potential for post-operative sensitivity but take on a much greater role long-term in serving as pulpal protectants.
Several qualities of a liner are necessary for effective pulpal protection: 1) establish a tight seal to prevent bacterial invasion; 2) stimulate mineralization; and 3) maintain an antibacterial alkaline-related biological environment.
Post-operative sensitivity is partially related to the remaining dentin thickness following cavity preparation and the presence of bacteria. There’s no material better to protect the pulp than dentin itself. The remaining dentin thickness between the base of the cavity preparation and the pulp is one of the most important factors in protecting the pulp from toxins. A 0.5 mm thickness reduces the effect of toxins by 75 percent. A 1.0 mm thickness reduces the effect of toxins by 90 percent. A 2.0 mm remaining dentin thickness or more results in little or no pulpal reaction. It is at this 0.5 mm region that liners become most important. Clearly, decreasing the remaining dentin thickness of cavity restorations can compromise odontoblast survival and influence repair in the pulp-dentine complex after injury.1
Related reading: How to cement a lithium disilicate restoration with eCEMENT™
Calcium hydroxide
Calcium hydroxide has been used as a lining material since the 1920s. Because of the basic pH of about 11, calcium hydroxide is both antibacterial and can neutralize the acidic bacterial byproducts. The high pH creates an environment conducive to formation of reparative dentin. In addition, calcium hydroxide has the capacity to mobilize growth factors from the dentin matrix, causing the formation of new dentin. Calcium hydroxide is an ideal lining material for the very deep cavity preparation and also continues to represent an option for a direct pulp cap.2
Adhesive resins
Adhesive resins contain acidic monomers that cause pulpal irritation. Many dentin bonding agents and resin reinforced glass ionomers are actually detrimental when placed on the pulpal tissues. In contrast, calcium hydroxide has been shown to provide a significantly improved potential for pulpal repair compared to adhesive resins.3
More from BISCO: BISCO introduces CORE-FLO DC LITE
Continue reading on Page 2 ...
Self-setting calcium hydroxide
Unfortunately, the self-setting formulations of calcium hydroxide are highly soluble and subject to dissolution over time.4 Traditional calcium hydroxide liners are easily lost during acid etching. Dentin bonding agents that contain water, acetone or alcohol can also detrimentally affect the properties of calcium hydroxide. Therefore, when a restoration of composite resin is planned, resin modified glass ionomer liners are required as a separate step to line the cavity preparation sealing over the calcium hydroxide material.5
Mineral trioxide aggregate
In recent years, mineral trioxide aggregate (MTA) preparations have been introduced. MTA materials are considered calcium containing silicate cements. The primary reaction of MTA calcium silicates with water is calcium hydroxide. These calcium silicate containing materials are also antibacterial, biocompatible, have a high PH and aid in the release of bioactive dentin matrix proteins. Significant disadvantages of self-cure MTA for the restorative dentist include the slow-setting times from several minutes to hours and high cost per use. As a result, two-step procedures are frequently necessary requiring interim restorations. Recent evidence indicates that an indirect pulp cap can be performed in a single treatment appointment.4
Related reading: How to bond a lithium disilicate restoration using BISCO eCEMENT
The solution
The most recent product to be introduced to the restorative dentist is BISCO’s TheraCal™ LC . This material is a light-cured, resin-modified calcium silicate lining material. In simplistic chemical terms, TheraCal LC offers the pulpal/dentin benefits of both calcium hydroxide and resin-modified glass ionomers in one product. The material demonstrates strong physical properties with low water solubility and can be light cured up to a thickness of 1.0 mm. Dentinal fluid absorbed by TheraCal LC results in the release of calcium and hydroxide ions. Calcium is necessary for rapid apatite stimulation and hydroxide ions are required for providing an “alkalinizing effect” for wound healing propagation. TheraCal LC is intended for use as an internally placed pulpal protectant liner over both occlusal and axial dentin. When performing a direct pulp cap, use of a rubber dam to reduce bacterial contamination, apex development and control of pulpal hemorrhage are among the essential factors for success.
More on BISCO: 7 clinicians discuss 7 bonding agents
Continue reading on Page 3 ...
Case presentation
The following case demonstrates the use of TheraCal LC as a lining material:
The patient presents with a mandibular premolar with a large distal carious lesion (Figs. 1 and 2).


Fig. 1
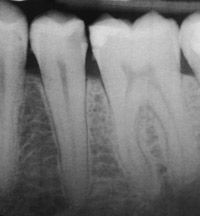


Fig. 2

The caries were carefully excavated resulting in a deep preparation, especially on the axial wall (Fig. 3).

Fig. 3

Related reading: How to simplify adhesive cementation with DUO-LINK UNIVERSAL™
A thin layer of TheraCal LC was placed on the dentin over the deepest portions of the preparation using the convenient syringe delivery system and then light cured for 20 seconds (Fig. 4).

Fig. 4

Excess liner was removed using hand instruments and the cavity preparation was etched, rinsed and coated with adhesive, which was air-thinned and light cured (Figs. 5 and 6).

Fig. 5


Fig. 6

Review: Why Catapult Group evaluators would convert to Bisco's DUO-LINK
Continue reading on Page 4 ...
The cavity preparation was matrixed (Fig. 7) and composite resin then syringed into the cavity preparation (Fig. 8).

Fig. 7


Fig. 8

References
1. About I, Murray PE, Franquin JC, Remusat M, Smith AJ. The effect of cavity restoration variables on odontoblast cell numbers and dental repair. Journal of Dentistry 2001;29:109-117.
2. Weiner R. Liners, bases and cements: material selection and clinical applications. Dent Today 2005 Jun;24(6):64, 66-72.
3. Modena KCS, Casas-Apayco LC, Atta MT, Costa CAS, Hebling J, Sipert CR, Navarro MFL, Santos CF. Cytotoxicity and biocompatibility of direct and indirect pulp capping materials. J Appl Oral Sci 2009;17:544-54.
4. Hilton TJ. Keys to clinical success with pulp capping: a review of the literature. Oper Dent 2009;34:615-625.
5. El-Araby A, Al-Jabab A. The effect of some dentin bonding agents on Dycal lining cement. Saudi Dental Journal 16(3):102-106.
6. Apatite – forming ability of TheraCal pulp – capping material. Gandolfi MG, Siboni F, Taddei P, Modena E, Prati C. J Dent Res 90(Spec Iss A):2520, 2011.
7. Chemical – physical properties of TheraCal pulp – capping material. Gandolfi MG, Suh B, Siboni F, Prati C. J Dent Res 90(Spec Iss A):2521, 2011.
Dental Innovator: BISCO eCement simplifies cement selection process










ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.






