How to maximize patient happiness with custom treatment options
Offering treatments plans that fit patient comfort levels can be the key to successful treatment.



In dentistry, there’s no such thing as a one size fits all approach to treatment. Even in every day procedures like deep caries restorations, some patients will have a better outcome with a full coverage crown and others may be just fine with a direct composite procedure. What may be a great option for one patient could be disastrous for another, so it’s important to always consider what the patient goals are for treatment.
Nowhere is this more prevalent than in a full-mouth reconstruction case. I could fill pages with the number of options dentists have for full-mouth restorations, but the most important factor to consider in these cases is the patient. Specifically, one should consider the patient’s diagnosis, their age, their financial situation, and their desired final esthetic outcome.
Since procedures like these require deep commitment by the patient, we would be doing them a disservice by not planning each case around their specific situation and only providing options that are easier to complete or will take the least amount of time.
In the following case, I could have chosen any number of different treatment options, from full-mouth crowns to reshaping each tooth with composite. The patient could have also chosen a number of treatment options, as he visited several different dentists to ensure he was receiving the care he felt comfortable moving forward with. In the end, he elected to move forward with my office because we came to a mutual understanding of what was desired and I was able to offer a treatment plan that fit within his comfort level.
Continue to the next page for the case study.



Case study
The patient, a 26-year-old male, had severe bruxing and over the course of eight years had worn his teeth down to 5 mm (Fig. 1). After an initial consultation, our team determined that given his young age, we wanted to be as conservative as possible. We felt confident we could achieve long-lasting, esthetic results by minimally prepping the teeth. We would only need to round the incisal edges and then bond veneers onto the upper and lowers.
The patient was excited to move forward with this option because it allowed him to reverse treatment at any point without the negative consequences of crown preparations. By considering the patient’s age and a myriad of options, we were able to come up with a treatment plan that the patient was comfortable with and that we were confident would provide him everything he wanted for his smile.






Step 1:
The teeth were left untreated and a preliminary impression was taken and sent to the lab. The lab created a wax up with new vertical dimensions and milled a continuous top and bottom temporary restoration out of PMMA (Fig. 2).



Step 2:
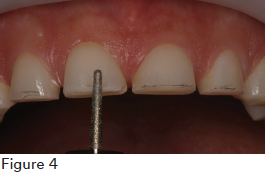
The temporaries were then tried in (Fig. 3) and a minor rounding was done to prepare each tooth (Fig. 4). This was done without any anesthetic, as the preparations were minimal.





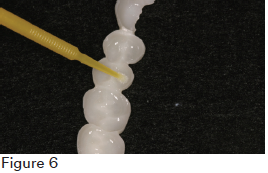
The temporaries were then air abraded and the teeth were spot etched. A thin layer of 3M™ ESPE™ Scotchbond™ Universal Adhesive was placed on the intaglio surface of the restoration and on the teeth (Figs. 5, 6).




The patient wore the temporaries for 12 weeks (Fig. 7) to ensure comfort with tooth size and shape.



Step 3:
Based on a prior impression, the lab created final restorations using IPS eMax for the upper arch (Fig. 8). The patient returned and after a try-in, the intaglio surface of the restoration was salinated and the entire preparation was etched (3M™ ESPE™ Scotchbond™ Universal Etchant). Scotchbond Universal Adhesive was then applied to the restoration and preparation. The final restoration was cemented using 3M™ ESPE™ RelyX™ Veneer Cement. Upon placement, excess cement was extruded from the restoration and was easily cleaned up. The same process was completed for the remaining teeth.






Conclusion:
The final restorations (Fig. 9) provided the patient with a smile he was proud to show off and it was completed using an extremely conservative treatment. The margins were supragingival due to the minimal preparation and undercut of the teeth and a very minor esthetic compromise was made in order to preserve tooth structure. This was augmentation, not amputation of the teeth. If the patient wants to reverse treatment in the future, he can do so without the negative consequences that would have occurred when bonding and cementing to dentin and the more aggressive preparations needed for crowns. The patient is planning to complete treatment on the lower arch at a future date.












Product Bites – November 10, 2023
November 10th 2023The weekly new products podcast from Dental Products Report is back. With a quick look at all of the newest dental product launches, Product Bites makes sure you don't miss the next innovation for your practice. This week's Product Bites podcast features new launches from Amann Girrbach, DMG, Pac-Dent, and ASI Dental Specialties. [4 Minutes]

ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.

Product Bites – October 27, 2023
October 27th 2023Product Bites makes sure you don't miss the next innovation for your practice. This week's Product Bites podcast features new launches from Kerr Dental, MGF, PreXion, ZimVie, Amann Girrbach, VOCO, ASI Dental Specialties, DMG, and NovoDynamics. [8 Minutes]



