How to create esthetic results using digital dentistry
Utilizing a digital workflow allows for the best implant position as well as the most optimum esthetics.


Digital dentistry is changing the way we practice implant dentistry - almost on a daily basis. The days where we brought our patients to surgery and placed the implant “where the bone was” are over. Doctors must now think of the final result first before they even place the implant. This includes not only planning the eventual tooth position, but the surrounding gingival topography as well.
Through the use of computer planning software, we can now consider the best implant position, which allows the most optimum esthetics. Now, doctors can include sculpting or developing the gingival contour as an integral part of their implant placement. Using a complete digital workflow, these steps are easily achieved to provide our patients with ideal implant placement as well as esthetic restorative considerations.
Trending article: The top 10 developments in dental technology in 2017
This technique starts with good diagnosis and treatment planning. Beginning with our clinical exam, we design our case with the end result in mind. A well-designed case, along with a well-designed provisional, will not only prepare the emergence profile prior to implant placement but will also assist the implant surgeon in choosing optimal implant position. When a cone beam computed tomography (CBCT) scan and a digital impression of the patient’s existing dentition are obtained, the goal is to create two files: the CBCT, which is a DICOM file, and the intraoral scanner file, which is in a STL format. We then merge those two files in an implant planning software to fabricate our guide and provisional restoration. If teeth are present, we can use these as guides to where we need to place our implants. If teeth are not present, then virtual teeth can be placed into the digital planning software so that implant position can be planned in an ideal location.
Typically, a surgical guide is printed next and temporary abutment and provisional restoration are milled from these digital files. This allows optimum implant placement as well as esthetic gingival contouring during the healing phase. We are starting to develop the emergence profile of the restoration to mimic that of a natural tooth by developing gingival contours through preplanned and pre-milled provisional restorations or gingival formers; inserted at the time of implant placement.
Continue to page two to read the case study...
Case study
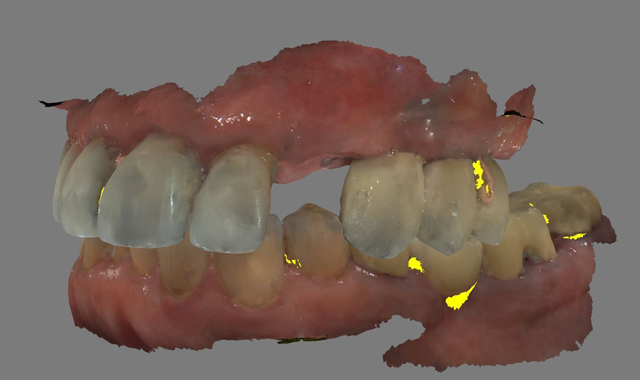
A 61-year-old male presented to my office with a fractured maxillary left canine. His past medical history was significant for previous DVT for which he was taking Coumadin. He has no known allergies (Fig. 1).


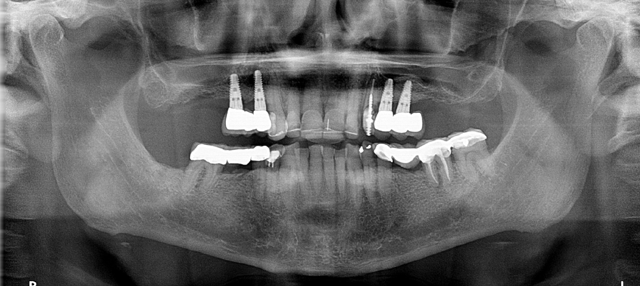


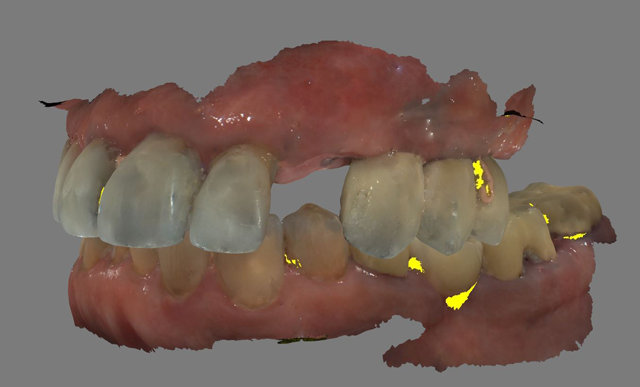
Fig. 1 Fig. 2
A CBCT scan was taken with a Carestream Dental CS 9300 (Figs. 2 and 3) and an intraoral scan was obtained using a Carestream Dental intraoral scanner (Figs. 4 and 5).






Fig. 3 Fig. 4
In this case, one file was sent to Roe Dental Labs in Ohio for fabrication of the surgical guide and another file was sent to Vulcan Dental Labs in Alabama for fabrication of a temporary restoration. The exactness of the digital technology allowed for this degree of specificity whereby both the guide and the temporary fit together as if they were made at the same lab (Figs. 6 and 7).

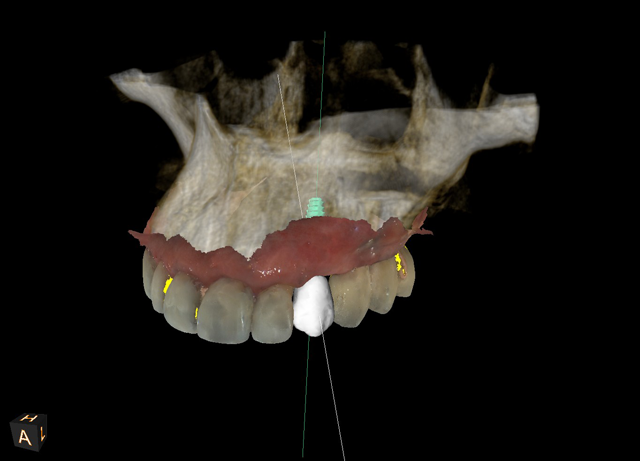



Fig. 5 Fig. 6
The patient was taken to the oral surgicenter where, under intravenous sedation, the maxillary left canine was surgically removed using appropriate periotomes and elevators. The tooth-borne surgical guide was placed (Fig. 8) and, using the Biohorizons Guided Surgical protocol, the Biohorizons Tapered Internal 4.6mm x12mm immediate implant was placed (Fig. 9). Ostell reading of 68 confirmed sufficient initial stability to provide an immediate load.






Fig. 7 Fig. 8
The Biohorizons custom milled temporary abutment and temporary custom PEEK crown were placed (Fig. 10). The gap between the implant and the extraction socket grafted with MinerOss, the occlusion adjusted and the soft tissue closed starting to contour the gingival tissues immediately.





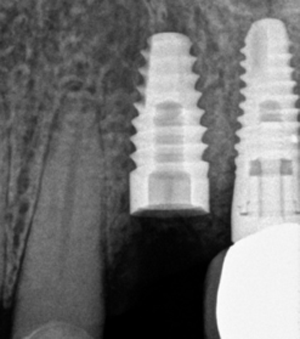
Fig. 9 Fig. 10
This technique utilizes a digital workflow to provide initial implant planning, placement and esthetic sculpting of the gingival tissues. It affords the ability to start contouring an ideal emergence profile at the time of implant placement (Fig. 11).


Fig. 11
The provisional crown will be in place for three months and, following Ostell testing again, a final restoration affording optimum tissue contour will be fabricated.
















ACTIVA BioACTIVE Bulk Flow Marks Pulpdent’s First Major Product Release in 4 Years
December 12th 2024Next-generation bulk-fill dental restorative raises the standard of care for bulk-fill procedures by providing natural remineralization support, while also overcoming current bulk-fill limitations.

