How to use TheraCal LC for direct and indirect pulp capping
A look at how Bisco's TheraCal LC could be used in your practice.



After more than five years of research and development, TheraCal LC was made available to clinicians in November 2011. It has been estimated that in the past three years, over five million restorations have been placed using TheraCal LC as a direct or indirect pulp capping material.
The popularity and rapid growth of this product has certainly surprised BISCO, launching it to be one of their top selling products. It is wildly popular for use as a direct pulp-cap, yet remains underutilized as an indirect pulp-cap. Perhaps this is because it requires a little more material in this procedure, or perhaps it is due to a lack of understanding of how TheraCal LC can assist in facilitating the formation of reparative dentin, improving the prognosis of this procedure.
Direct pulp-capping
There are three types of pulp exposures: carious, mechanical and traumatic. Both mechanical and traumatic pulp exposures can be easier to treat due to their higher success rate. However, the carious exposure remains difficult to treat based on the level of pulpal inflammation and infection. Due to the often unpredictable pulpal response to direct pulp-capping of carious exposures, many clinicians opt for providing endodontic therapy every time the pulp is exposed. However, if the exposure is small and the pulpal status has been properly diagnosed, many clinicians are also finding success with direct pulp-capping by using TheraCal LC.
Rarely does a clinician diagnose the pulpal status of a tooth prior to providing routine restorative fillings. Either a clinical or radiographic exam reveals the need for a direct filling. It should be recognized that the level of infection is frequently deeper than what a radiograph can provide. In addition, it is usually not until after the pulp is exposed that a clinician diagnoses the tooth as being either symptomatic or asymptomatic reversible or irreversible pulpitis. Regardless, it is the best practice to avoid exposing the pulp entirely unless there are clear indicators for providing root canal therapy.
Indirect pulp-capping
Knowing when to stop removing carious dentin can be difficult, especially when the exact location of a pulp horn or chamber is not known. Most clinicians rely upon tactile sensation or the hardness of the dentin to determine when to stop excavating. When near the pulp, it is advised to stop excavating and leave a layer of affected dentin.
This affected dentin may be demineralized and softer than sound dentin, but preserves the collagen structure, lacks contamination with bacteria, can extend up to one mm and is capable of remineralizing. In contrast, infected dentin is softened dentin (demineralized and destroyed collagen) that remains infected with bacteria, and should be removed.
The procedure by which incomplete excavation is provided, leaving a thin layer of affected or sound dentin when near the pulp, is called an indirect pulp cap. This procedure is usually more successful than a direct pulp cap, and can provide the tooth the opportunity to repair itself and maintain vitality.
However, it has fallen out of favor with the introduction of self-etching adhesives, the additional cost of the indirect pulp capping material, and the lack of insurance reimbursement. It should be noted that adhesives are acidic, do not disinfect the dentin and do not provide the necessary chemicals for tooth remineralization. Providing an indirect pulp cap and/or liner with TheraCal LC has many benefits, that when combined with a well-sealed restoration, can allow the tooth many more years of service prior to endodontic treatment.
TheraCal LC

Chart 1
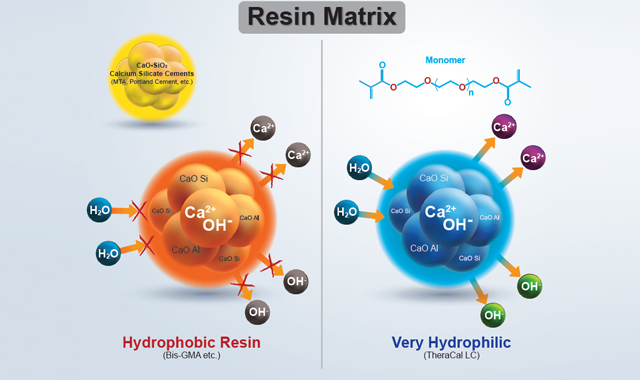
TheraCal LC is a light-cured, flowable resin-modified calcium silicate filled liner that can be used for direct and indirect pulp caps. TheraCal LC possesses many of the same beneficial properties similar to other commercially available self-curing MTA products. TheraCal LC’s proprietary resin formula consists of tri- and di-calcium silicate particles in a hydrophilic monomer that provides significant calcium and hydroxide ion release (Chart 1). These ions serve many roles in the ability to remineralize tooth structure via apatite formation in an alkaline environment. Stable and durable as a liner, base or pulp-capping material, it is permeable to dentinal fluid but resists dissolution.
TheraCal LC may act as a scaffold for reparative dentin formation. Dentinal fluids are absorbed within it, resulting in the release of calcium and hydroxide ions, and the tooth responds to form apatite and a bond, supporting the natural sealing ability of the product. This ability to assist in the formation of apatite plays a critical role in pulpal protection.
Technique for TheraCal LC
- Isolate the tooth to be treated with a rubber dam. Research still indicates that this is the best technique to use.
- Excavate all infected dentin and leave a thin layer of affected dentin when near the pulp. Use maximum caution to avoid exposing the pulp.
- Clean the cavity with 2% chlorhexidine (Cavity Cleanser). Use a moist cotton pellet for at least 20 seconds.
- If a pulpal exposure occurs, control hemorrhage with sterile saline, chlorhexidine or sodium hypochlorite.
- Apply TheraCal LC to the pulpal floor of the prepared cavity up to 1mm. This will assist in reducing post-operative sensitivity via insulation. Make sure to apply to TheraCal LC to moist dentin as this will improve its initial bond and stability.
- Light-cure TheraCal LC for 20 seconds. TheraCal LC is very opaque and requires a full cure.
- Selective etch the enamel (Select HV Etch) or total-etch the entire preparation.
- Apply adhesive (All-Bond Universal).
- Fill preparation with restorative material of choice (composite, amalgam, core-buildup, etc.).
- Shape, finish and polish restoration.
- Seal tooth-restorative margins with BisCover LV.
Clinical Captions-dentistry courtesy of Dr. Ross Nash
- Distal-occlusal caries present on an asymptomatic mandibular first premolar.
- Incomplete excavation of caries leaving affected dentin without exposing the pulp.
- Direct placement of TheraCal LC as an indirect pulp cap on entire pulpal floor.
- Thin layer of TheraCal LC after light-cure of 20 seconds.

Fig. 1


Fig. 2


Fig. 3


Fig. 4

Key features and benefits of TheraCal LC
- Significant calcium1 release stimulates hydroxyapatite formation, secondary dentin bridge formation2,3, and leads to a protective seal5.
- The alkaline pH (hydroxide ions) promotes healing2,4 and contributes to pulpal repair and apatite formation.
- Forms a protective barrier5 that insulates the pulp (which may lead to less tooth sensitivity).
- Moisture tolerant with very low solubility1.
- High radiopacity making it easily identifiable on radiographs.
- Light-curable with immediate set and very easy to use.
- Strong physical properties6 to withstand the forces of mastication under composites, amalgams, cements and other base materials.
- Flowable, yet stays where it is placed.
References
1. Gandolfi MG, Siboni F, Prati C. Chemical–physical properties of TheraCal, a novel light-curable MTA-like material for pulp capping. International Endodontic Journal. 2012 Jun;45(6):571-9.
2. ADA definitions for direct and indirect pulp capping at http://www.ada.org/en/publications/cdt/glossary-of-dental-clinical-and-administrative-ter
a. direct pulp cap as a “procedure in which the exposed vital pulp is treated with a therapeutic material, followed with a base and restoration, to promote healing and maintain pulp vitality.”
b. indirect pulp cap as a “procedure in which the nearly exposed pulp is covered with a protective dressing to protect the pulp from additional injury and to promote healing and repair via formation of secondary dentin.
3. Apatite-forming Ability of TheraCal Pulp-Capping Material, M.G. GANDOLFI, F. SIBONI, P. TADDEI, E. MODENA, and C. PRATI J Dent Res 90
(Spec Iss A):abstract number 2520, 2011 (www.dentalresearch.org)
4. Okabe T, Sakamoto M, Takeuchi H, Matsushima K (2006) Effects of pH on mineralization ability of human dental pulp cells. Journal of Endodontics 32, 198–201.
5. Sangwan P; Sangwan A; Duhan J; Rohilla A. Tertiary dentinogenesis with calcium hydroxide: a review of proposed mechanisms. Int Endod J. 2013; 46(1):3-19
6. Mechanical Properties of New Dental Pulp-Capping Materials Over Time. M. NIELSEN, R. VANDERWEELE, J. CASEY, and K. VANDEWALLE, USAF, JBSA-Lackland, TX, , J Dent Res 93(Spec Iss A): 495, 2014 (www.dentalresearch.org)










Henry Schein Now Exclusive Distributor of Curodont Remineralization Solution to DSOs
September 19th 2024The company announced it has reached an agreement with vVARDIS to serve as the exclusive distributor of their drill-free Curodont™ Repair Fluoride Plus product to larger dental service organizations in the U.S.




