10 of the CRAZIEST impressions you've ever seen
Talk to any group of dental technicians about their biggest work frustrations, and chances are, it won't be long until people start talking about impressions. These are some of the worst.



Talk to any group of dental technicians about their biggest work frustrations, and chances are, it won’t be long until people start talking about impressions.
If you work in a lab, you’ve already thought of an impression you saw you could scarcely believe-either for how poorly it had been done, how much discomfort it must have caused for the patient and just … how weird it was.
3 products that can help your clients take better impressions
With that in mind, we wanted to hear stories from technicians who have seen it all-and hear their stories of the craziest impressions they’ve ever seen. Here’s what they told us:
Mark Ferguson, Core3dcentres: In one case I remember, we had a full arch impression come into the lab with vomit impregnated in the PVS material.
A new study: Edentulism can affect success of impression techniques


Dr. DiTolla reminds dentists: Blood + impression material = bad times
Dr. Michael DiTolla, Glidewell Laboratories: When you look at this impression (image above), at first glance, you can see the patient has a wisdom tooth. The doctor did manage to get a wisdom tooth in the impression tray, which is nice, but it looks like there is a big pull on the lingual. Upon closer look, we can see that there is somewhat of a margin, and then everything just stops. There seems to have been a huge channel of blood. These impression materials worked so well on every tooth except the one that was prepped. That is one of the consequences when you have gingiva that’s bleeding.
Dr. David S. Hornbrook, Keating Dental Arts: Having been involved in dental education the past 25 years and receiving emails and photos from doctors and laboratories that were having concerns with impressions, I thought I had seen it all until recently. We have some unbelievably great clinicians sending their work to Keating Dental Arts, and then we have some that need some guidance. One [recent case] was a difficult full mouth rehabilitation case that included altering Vertical Dimension. Instead of taking accurate full arch polyvinyl maxillary and mandibular impressions and an accurate bite registration with a face bow transfer jig, we received three sepa rate Triple tray quadrant Impressions: A ½ arch triple tray for the right side, ½ arch triple tray for the left side, and a small anterior triple tray. The doctor wanted us to pour these up separately, somehow join them together and make a full arch model and then open vertical from this pre-existing position. The model department at Keating is amazing and somehow they pulled it off because we fabricated the case and the doctor emailed us and said it went great.
Step-by-step: An ideal implant bridge


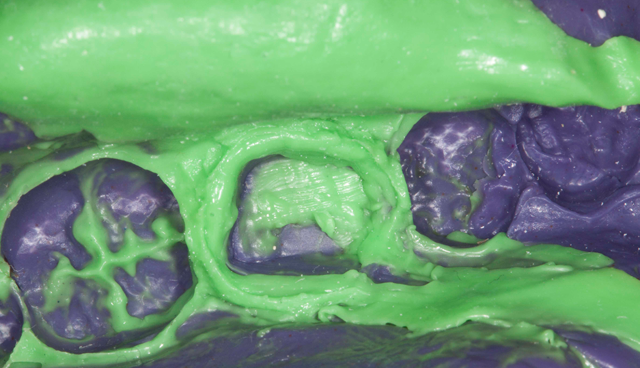
When the patient bites the tray ...
Dr. Michael DiTolla: Here’s an impression (see above) where we have a wisdom tooth and it’s not contained in the impression; it’s actually biting down on the tray itself. That makes it a little difficult for this impression to work. When we look a little bit closer, we can see extra material hanging off, unclear margins, big divots in the margin itself, and just a huge void right at the margin. If you don’t take care of the tissue and it starts to bleed, these impression materials will not work. They will not set well. They’ll get pushed out of the way by the blood. This impression is a really good example of that.
Mark Ferguson: We had a upper full PVS impression that the extra material sticking off the back of the tray was a good 4 inches of a clear impression of the patients throat. We were surprised this one did not have an vomit on it!



Who knows what those specks are?
Dr. Michael DiTolla: When you look at this impression (above), you can see two bicuspids prepped in this double-arch tray. Zoom in, and you can see where it looks like extra material was just added on at the end. We’ve got a little tear as well; not the end of the world, but again, just overall not a lot of detail. You can really see what a mess this impression is toward the front. We have some white speckles here. Maybe it’s latex. It’s difficult to see. This is going to be a really hard one.
Dr. David Hornbrook: A second case that we were not able to save involved a clinician using Alginate as the heavy body and a polyvinyl as the light body in a quadrant impression. It was sent from out of state, so by the time we received it, the alginate had dried up and lifted from the tray and the light body was no longer attached to the alginate. We’re good, but not that good! Of course, when we called the doctor, he blamed his dental assistant.
The List: 6 benefits of digital impressions and a model-less workflow


Wait, are those teeth or did a pencil fall in the impression material?

Dr. Michael DiTolla: These are some anterior preps as you can see (in the image above) on the front, and they look pretty indistinct. You can see some rough outlines of what appear to be teeth; some kind of round, prep-like shapes. Looking a little bit closer, it doesn’t look like there was any retraction cord or diode laser used here. It’s unclear what was used. In fact, we’re not even sure the teeth were necessarily prepped. It just looks like there was an impression of some tiny teeth. If we flip the impression over and look at it toward the lingual, you can see that we really don’t have much definition there either. But at least we can tell they’re preps because we see some of the diamond marks in there. This impression had to be sent back pretty quickly. There’s one tooth toward the posterior that you can almost make out the margins and where the tooth is, but the rest of it is just kind of sloppy.
Mark Ferguson: While not strictly an impression, we did have a case come in that the prescription was completely filled out, then covering the full front of it was written "HIV POSITIVE" in bold red sharpie. We could still read the Rx, which we thought was interesting because this particular doctor was known for the old "call me" instructions on all of his cases.



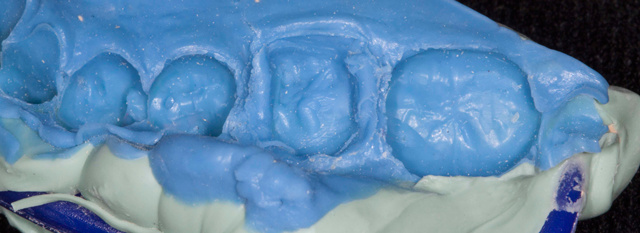
One doctor apparently thought, "a model molar is good enough!"
Dr. Michael DiTolla: This one (photo above) is really confusing because when you look at this impression, it’s got some really sharp angles on it, and you can tell there’s no patient whose mouth actually looks like this. Based on this 90-degree angle and how smooth it is, it looks like a polyvinyl impression of a model that has a base formed on it. This causes us to say, “Wait a minute: This wasn’t taken in a human mouth, yet it appears to be an impression of a human molar.” It has this big band around it that kind of looks like the margin, but it’s not. The margin is that thin line down below it. As you look at it from multiple angles, it’s really tough to figure out what happened. Apparently, the doctor took an impression of a model, and then he relined it with light-body material. It doesn’t look to be like it was done in the mouth; it looks like it was done on a model. Frankly, it’s really confusing, and we’re not sure what to make of it. It’s really just kind of crazy when you look at it and see exactly what’s going on.
All photos (including top photo) courtesy of Dr. Michael DiTolla/Glidewell Laboratories.









